Association of National Initiatives to Improve Cardiac Arrest Management With Rates of Bystander Intervention and Patient Survival After Out-of-Hospital Cardiac Arrest
JAMA. 2013;310(13):1377-1384. doi:10.1001/jama.2013.278483.
https://jama.jamanetwork.com/article.aspx?articleid=1745678
This study released in 2013 analysed the improvements made to out of hospital cardiac arrest survival rates in Denmark between 2001 and 2010. The improvements made in 30 day and 1 year survival were due to several measures, including an emphasis on bystander CPR training. The other measures included:
(1) Implementation of mandatory resuscitation training in elementary schools (since January 2005), as well as when acquiring a driver’s license (since October 2006), combined with an increase in voluntary first aid training;
(2) The free distribution of approximately 150 000 CPR self-instruction training kits between 2005 and 2010;
(3) The nationwide improvement of telephone guidance from emergency dispatch centers to bystanders witnessing a cardiac arrest, including the addition of health care professionals at dispatch centers, starting from 2009;
(4) A large increase in the number of automated external defibrillators located outside hospitals (approximately 15 000 were in place by 2011);
(5) Efforts to improve advanced care with updates of clinical guidelines, including introduction of therapeutic hypothermia starting from 2004, and increasing focus on early revascularization; and
(6) Overall strengthening of the EMS system with training of the ambulance personnel, including implementation of paramedics, mobile emergency care units staffed with specialized anesthesiologists dispatched as rendezvous with basic life support ambulances, or both.
What can be done in Australia, based on this study?
(1) Implementation of mandatory resuscitation training in elementary schools (since January 2005), as well as when acquiring a driver’s license (since October 2006), combined with an increase in voluntary first aid training;
(2) The free distribution of approximately 150 000 CPR self-instruction training kits between 2005 and 2010;
(3) The nationwide improvement of telephone guidance from emergency dispatch centers to bystanders witnessing a cardiac arrest, including the addition of health care professionals at dispatch centers, starting from 2009;
(4) A large increase in the number of automated external defibrillators located outside hospitals (approximately 15 000 were in place by 2011);
(5) Efforts to improve advanced care with updates of clinical guidelines, including introduction of therapeutic hypothermia starting from 2004, and increasing focus on early revascularization; and
(6) Overall strengthening of the EMS system with training of the ambulance personnel, including implementation of paramedics, mobile emergency care units staffed with specialized anesthesiologists dispatched as rendezvous with basic life support ambulances, or both.
What can be done in Australia, based on this study?
- Mandatory CPR training in schools and when acquiring a Drivers License - this is a grass roots measure will set the next generation up to have some understanding of resuscitation and increased awareness of bystander involvement.
- Free Distribution of CPR self-instruction packs - while this measure may reach some people who may not otherwise engage in CPR training, there has been no proper evaluation of the effectiveness of resuscitation learnt by this method when applied to an actual patient.
- The nationwide improvement of telephone guidance from emergency dispatch centers to bystanders witnessing a cardiac arrest, including the addition of health care professionals at dispatch centers - there is a variance in Australia between the systems, quality and staff used in emergency dispatch to provide telephone guidance in cardiac arrest. some services use clinical personnel for this critical advice, other use scripted dialogue given by non-clinical call-takers. Scripted advice does not differentiate between types of cardiac arrests or the individual/s providing assistance at the scene. SCA advice should be limited to chest compressions based on unconsciousness (no response to pain) and abnormal breathing and advice on ventilation should be restricted to paediatric and other hypoxic arrests.
- A large increase in the number of automated external defibrillators - this is a fundamental difference between Australia and other countries in improving cardiac arrest outcomes. In Australia we have no WHS rules that make industry and public buildings install AEDs. There is currently no imperative for general practices and medical centers to have an AED under national accreditation standards. There is also no government initiatives to educate the public about the importance of early defibrillation, empower them to use public access defibrillators and highlight the steps. Both Federal and NSW Health Ministers are not interested in the more than 500 people a week that suffer SCA and would rather focus on strategies to prevent death in much smaller causes of death and disability.
- Efforts to improve advanced care with updates of clinical guidelines, including introduction of therapeutic hypothermia and increasing focus on early revascularization - Ambulance services in Australia are still experimenting with hypothermia but have made in-roads in the area of pre-hospital antii-thomboloitic therapies. There is more room for bolder approaches to innovation in pre-hospital care rather than being driven by hospital-based specialists or dogmatic consensus opinions of the ARC.
- Overall strengthening of the EMS system with training of the ambulance personnel, including implementation of paramedics, mobile emergency care units staffed with specialized anesthesiologists dispatched as rendezvous with basic life support ambulances, or both - Australia has had ACLS Paramedic systems for several decades. The population distribution and distances in Australia preclude widespread specialised resuscitation units, however in large, densely populated urban areas the establishment of cardiac arrest EDs may be viable.
Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials
BMJ 2003; 327 doi: http://dx.doi.org/10.1136/bmj.327.7429.1459 (Published 18 December 2003)
Objectives To determine whether parachutes are effective in preventing major trauma related to gravitational challenge. Design Systematic review of randomised controlled trials.
Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; appropriate internet sites and citation lists. Study selection: Studies showing the effects of using a parachute during free fall.
Main outcome measure Death or major trauma, defined as an injury severity score > 15.
Results We were unable to identify any randomised controlled trials of parachute intervention.
Conclusions As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomised controlled trials. Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute.
Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; appropriate internet sites and citation lists. Study selection: Studies showing the effects of using a parachute during free fall.
Main outcome measure Death or major trauma, defined as an injury severity score > 15.
Results We were unable to identify any randomised controlled trials of parachute intervention.
Conclusions As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomised controlled trials. Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute.
The use of expert consensus opinion as strong evidence in the absence of evidence; is this sound methodology?
A discussion, using the example of the Australian Resuscitation Council (ARC) in the formulation of recommendations and guidelines relating to resuscitation.
Author: S. Gould 2016
Aim
The purpose of the paper is to discuss the issues resulting from the use and reliance on expert consensus opinion (referred to in Australian Resuscitation Council or ARC literature as Level of Evidence IV or LOE IV). Further this paper will discuss errors in methodology and interpretation that may and do result in, less than ideal, recommendations in resuscitation practice, especially at BLS level; recommendations that are then implemented verbatim by the end-user, in the mistaken belief that they all represent “best-practice”. This can result in a lack of innovation and a stagnancy or degradation in positive outcomes, without appropriate accountability.
Background
The Australian Resuscitation Council (ARC) is an independent, private, voluntary, non-profit organisation that has representative members from key resuscitation related organisations. These members use a methodology that includes a reliance on Level of Evidence IV – Expert Consensus Opinion (both internally from the International Liaison committee on Resuscitation - ILCOR). While some of this expert opinion in harmonious, some is out of step with current international practice and expert opinion. The constitution of the organisation states that no responsibility is taken for any harm caused by the use of the consensus guidelines and that any recommendation does not mean that any other techniques are ineffective.
ARC LOE IV consensus opinion comes from at least two sources derived from international experts and LOE IV based on a re-analysis by local experts based on a local interpretation of the evidence. These two positions may be substantially different and may be contradictory but are presented as being equally rigorous in their position. This raises an important question about the status and methodology in the formulation of a consensus recommendation based on opinion and how two rigorous methodologies can result in differing end-points. For the individual or group seeking the best advice on which to base their guidelines this situation can be confusing, anomalous and illogical. Classes of LOE IV reflect degrees of confidence in the opinion, but all are presented as “best practice”. The methodology relied upon is that LOE IV is ranked by the evidence influence and therefore is of varying veracity. In actuality, the outcome is the same i.e. it is still a somewhat subjective opinion based on a review of selective research, including the decision to include or reject evidence and the personal opinions of those that make up the expert group. Therefore the LOE IV cannot take on the rigour of the considered evidence. In circumstances where the evidence is weaker the subjectivity increases and the associated rigour and veracity decreases. This variation at the end-user/implementer level is not distinguishable and one would naturally assume that all recommendations are equal in rigour.
Underlying expert consensus opinion using a specific methodology there must be to innate belief that anyone using the same methodology would arrive at the same recommendation. In a general sense this is what one should expect. Whilst this may be true where there is a wide variety of high level research and evidence, the same cannot be said at the other end of the continuum where evidence is weak or inconclusive and where a range of recommendations may reflect and suitably address the evidence. The assumption that is therefore made is that to reach any other conclusion is not scientific and therefore cannot contain any intrinsic value and therefore cannot and will not be considered. This flaw, based in attitude and belief in infallibility of process/ judgement/ methodology is central to much of the latency in the ARC BLS recommendations.
Discussion
Much of resuscitation practices (particularly BLS), have very little targeted and definitive research and so recommendations are determined (for the large part) on low, poor, weak or no direct evidence. Rarely is there such overwhelming strong evidence that one approach is clearly to be used at the exclusion of all others. In this vacuum LOE IV (expert consensus opinion) is used as a substitution and/or a subjective opinion of the conflicting evidence. However, an error in methodology occurs when change or alternate opinion is raised, in that those providing the consensus opinion (LOE IV) now consider that in order to alter their position there is a requirement for strong evidence (i.e. higher than LOE IV). This flaw in process now means that LOE IV has been inappropriately elevated in the evidence hierarchy to an unjustified superior position, presumably based on the level of evidence used to influence the opinion. However, even if influenced by higher levels of evidence i.e. based on strong evidence, as LOE IV it still only represents a subjective interpretation, at a point in time, it cannot assume the status of the underlying influence. It also means that the power of veto in consideration of any evidence is apportioned to the creators of the LOE IV (consensus opinion). This does seem on any level to be a significant flaw in the use of research methodology. Expert opinion can in some instances, be based on, the “discussion” section of a research paper rather than originating from the “conclusion” section, however both are not equal as evidence. Long periods between reviews can also confound the ability of opinion to keep pace/ consider the outcomes from changes in practice recommendations. In fact, proof of efficacy in practice is rarely (if ever) considered or studied as part of this methodology as proof and is not considered necessary and until studied at a formal/ high level (e.g. RCT) it is not taken into account. The history of resuscitation practice is littered with techniques based on expert opinion based on “studies” that were obviously ineffective (and sometimes dangerous) long before expert opinion was changed. As one observer rightly pointed out there are no RCT’s to support the use of parachutes when jumping from a plane and therefore we are totally reliant on informal observation to confirm the benefit over not using a parachute.
In reality, LOE IV is only a substitute for a collection of other evidence (weak and strong) that can be interpreted and/or result in opinion-based implementation strategies. It has little intrinsic merit over any other opinion or approach resulting from a consideration of the available evidence.
LOE IV “evidence” is not at this level in all research hierarchies. For example if we look at Joanna Briggs Institute Levels of Evidence, http://joannabriggs.org/assets/docs/approach/JBI-Levels-of- evidence_2014.pdf we see that consensus opinion by a single expert or a group of experts appropriately sits at Level 5 in the hierarchy i.e. the lowest level, sitting behind any other evidence levels. Likewise in the realms of Level 5 evidence it is only the self-assessed status of those who provide the opinion that guides those seeking direction. Regardless of the source of influence of the consensus opinion, it does not change its position in the hierarchy.
A confounding issue resulting from this self-assessed “expert” status (used in the formulation of consensus view) is each “expert group” can and does claim its own consensus opinion as an absolute and fundamental truth and tends to defend the ownership of this opinion against any contrary observation or ideas that threaten the authority and status perceived to be ascribed to self-assessed “expert opinion”. This is, of course, is not true of all expert groups, however it is certainly the case in Australia. Although this behaviour can and is frequently denied, actions are a better test of character. The close observer will see as a result, contradictory actions and statements that result from this duplicity of motivation. An example from our ARC example is the organisational slogan “Any attempt at resuscitation is better than no resuscitation”. This statement would appear to encourage an individual (particularly the un-trained bystander) to utilise any means they believe is appropriate in an attempt to save a life i.e. “at least one is trying”. The reality of the meaning of this statement is somewhat different and is clearly demonstrated in defensive actions when alternate recommendations are suggested. The actual meaning is “Any resuscitation that follows the ARC recommendations, including its own expert consensus opinion should be attempted; if unable then no resuscitation is better”. This contradiction in statement vs attitude is only supported by the flawed LOE IV status interpretation which we are discussing in this document. Interestingly, the disclaimer used on each recommendation obviates any responsibility for harm or failure of the recommendations to provide the expected outcome and recognises other methods may be of equal or better efficacy. These two statements are essentially and fundamentally contradictory.
The second statement made by the ARC is a disclaimer to the effect that they (the ARC) are not saying that there recommendations are relevant for all circumstances and that individuals should seek “specific advice” in deciding on methods that are applicable to their specific circumstances. Logically, this “specific advice” cannot be from the ARC as it has already (by this statement) referred readers away from the guidelines for advice. Therefore, presumably the statement refers to other sources and/or one’s own review of evidence and recommendations i.e. opinion of relevance. So why do we see such a strong defense of ARC consensus opinion if readers are encouraged to form an opinion independently of the ARC? This statement vs action is also illogical and contradictory in the defense of low level of evidence and demonstrates a misuse of expert opinion.
The other weakness of dogma in local, consensus opinion based recommendations is that the individual agenda of those constituting the expert group can more easily become part of the consensus without the need for the same rigour expected of external potential contributors to the collective opinion. Let us review an example that has been in question for more than a decade. The example from ARC literature is contained in Section 4 – Airway, where recommendations are listed for the management of upper airway obstruction (UAO). Of particular interest is the specific management of an upper airway obstruction (UAO) in the conscious patient. Firstly let us paraphrase the consensus opinion of the ARC and compare this with that of ILCOR and the international resuscitation expert community which includes bodies such as the ERC and AHA.
1. ARC – measures for the relief of UAO include firstly back blows and then “chest thrusts” followed by CPR if unconscious. The recommendation excludes the use of abdominal thrusts and refers to a small, single, yet unrelated postmortem study comparing CPR in a supine position with abdominal thrusts in a living patient.
2. The international resuscitation community – measures for the relief of UAO include firstly back blows and then chest and/or abdominal thrusts, followed by CPR if unconscious. Abdominal thrusts are considered to the most effective technique after the failure of back blows.
Before examining how consensus opinion can have these fundamental differences it is important to note that “chest thrusts” as mentioned in both consensus statements are not equivalent. The technique described by the international resuscitation community is a modified abdominal thrust method suitable when a patient is too large (including pregnancy) to attempt abdominal thrusts. The technique is performed standing behind and against the back of the patient and using two hands pulling toward the centre of the patient’s chest. This technique, as with abdominal thrusts, is supported by respiratory studies that show pressure changes induced in the airway as a result of utilising this technique. Whereas, the “chest thrusts” as described in ARC literature is a modified, single-handed CPR compression technique, that has no supporting respiratory studies or clinical trials.
In terms of our discussion around the use of LOE IV evidence, how did we get to this position that has resulted in a differing recommendation from not only the international resuscitation community, but practice across the world and more importantly after more than a decade no documented cases of success i.e. proof of efficacy. There are several factors that have contributed to this disparate, flawed and unchangeable position.
The ability of expert opinion (LOE IV) to be the re-interpreted by other expert opinion without a need for stronger evidence to support a different outcome. A test consensus opinion does not have to achieve.
The inappropriate direct substitution of unlike terms (such as “chest thrusts) to support a personal view/ opinion and thus take advantage of the outcome and reputation of evidence relating to the original technique without the need to support (with evidence) a experimental method.
The positioning of LOE IV evidence in an artificially elevated position so that strong evidence is required for change, even though the consensus opinion is based on weak, no or poor evidence or borrows rigour from an unrelated finding. This is true regardless of the source influence.
A deliberate dismissal of abdominal thrusts, based on an incomplete consideration of the evidence and a disproportionate emphasis on a misrepresented an “unacceptable risk” (a risk mitigated appropriately and considered against benefit by the international resuscitation community, including ILCOR). The only reason for this position therefore has to come primarily from a personal view of the experts that have contributed to the local expert opinion.
The vehement defense against alternative, (but equally or better evidenced) alternative opinions on the basis that LOE IV evidence has a status above its logical and justified level in research methodology.
A lack of an experimental framework and associated methodology when recommendations are clearly speculative.
What is the result of this difference in consensus opinion? Does it make a difference at the end-user level i.e. to the patient? And what feedback loops are in place to provide proof that one opinion turned out to be better than another? If we review the case of UAO as an example of a divergent view by experts on measures to address the same problem we can see the issues. In Australia an experimental modified chest compression technique and in the rest of the world abdominal thrusts and/or modified abdominal thrust on the chest. Since its inception in 1974 abdominal thrusts in the US have been credited anecdotally by the Washington Post with more than 100,000 saves, whilst in Australia after more than a decade using a different regime there are no documented cases of success. In the recent example in Western Australia a 2 ½ year old child who died after choking on a bubble gum ball he found in his stroller. This was a tragic outcome for the family and those involved and it is uncertain if any measures on the day would have relieved this obstruction. However, what is clear is that in compliance with local expert consensus opinion, 3 separate rescuers (these included a pharmacist, St John Ambulance Volunteers and St Ambulance – State Ambulance) were restricted from using abdominal thrusts and were only able to utilise an experimental technique with little if any supporting evidence (in either clinical trials or field application). The question that should be addressed first is to where in an “all care and no responsibility” methodology does responsibility for review lie. It is doubtful that (unlike an organisation in the general health sector ) that an ARC review (or RCA) of the circumstance has or will take place or seen as necessary in accountability. Differences in recommendations are not restricted to UAO and we see high level guidelines (like BLS Resuscitation) remaining to be focused on a sentimental but uncommon form and cardiac arrest i.e. the hypoxic arrest. This strategic direction, protected by an assumed rigorous methodology, cannot demonstrate improvements in outcome over SCA centered BLS guidelines but cannot be challenged.
Finally, there may be another reason why expert opinion can be at odds with “best practice” or other expert opinion and this relates to ideological and political pressures being brought to bear in the process. Political pressure can arise from dependent organisations, which have an interest in resisting change and the associated costs and imposition of implementing change i.e. the opinion to change can be delayed or moderated as a compromise. Ideological pressures can come from an unwillingness to “confuse” a long term message with change. This assumes that the lowest common denominator (e.g. BLS) is incapable of grasping a new focus or deciding between management options in an emergency. Whilst these pressures can be real considerations in recommendation and guideline development they only gain a controlling power at the LOE IV level where they can build legacy characteristics into recommendations and support sub-optimal guidelines.
Recommendations
The reality in the field of resuscitation is that as we learn more, there will always be better methods being developed than the accepted status quo. They can represent equal levels of opinion and evidence base. The misapplication and defense of any low ranked LOE IV can significantly hamper progress and innovation in guideline development. More significantly it can lead to an unfortunate regression in positive outcomes, when this flawed research methodology is used in resuscitation practice. Recommendation for improvement can be summarised as follows:
1. The adoption of a more appropriate evidence hierarchy system e.g. JBI - Levels of Evidence would more appropriately relegates and classifies consensus opinion. Additionally, nomenclature must clearly differentiate between opinion status and experimental recommendations.
2. Bodies utilising an evidence hierarchy as the basis for any recommendations must exercise appropriate diligence in ensure individual opinion does not unduly affect the consensus view.
3. Ethical and procedural practices need to demonstrate the appropriate and honest representation of research and evidence. The practice of “stolen rigour” used to substitute evidence from unrelated sources must cease immediately, to ensure the maintenance of reputation of expert panels.
4. All consensus opinion based guidelines must be appropriately open to general external scrutiny and peer review and an opportunity for input into development; at any time during the revision cycle. Consultation and comment must represent more than nominal achievements but an important and necessary pathway to excellence.
5. Effective and transparent mechanisms need to be in place to ensure ethical and scientific principles are central to process i.e. that processes are not inappropriately biased toward or away from recommendations for other reasons than a “balance of evidence”.
6. Internal policies that attribute inappropriate status to expert consensus opinion i.e. demand unnecessarily high levels of evidence to affect change; are unscientific and impediments to innovation and improvement.
7. The implementation of an experimental framework and methodology to appropriately manage speculative opinion based recommendations. This framework must necessarily include processes for the evaluation of efficacy to inform change, termination or progression. The use of LOE IV rather than an experimental methodology cannot obviate all responsibility. An experimental framework could allow for the appropriate assessment of regimes or procedures that are currently experimental in nature (due to being significantly different to international consensus opinion) and provide a platform for innovation in the area of resuscitation.
8. Expert consensus opinion should be constructed in consultation with a wider and sector specific group rather than cascading down from higher clinical levels under the assumption that there is an innate understanding of lower levels and their specific implementation/ interpretation challenges. This assumes expert status by inference rather than direct and relevant experience.
9. Any defense of consensus opinion should be done through appropriate debate and dialogue. Strategies such as “refusal to engage” and the “discrediting of individuals” are not appropriate strategies in the consideration of research/ evidence and the formulation of widely utilised guidelines and demonstrate a dedication to power rather than outcome.
10. Those assuming responsibility for guideline development (particularly those based on local consensus opinion) must accept some level of responsibility for the monitoring of efficacy, particularly if unwilling to commit to continuous development. Specifically, if an instrument assumes or has claim as “the authority” which results in others being forced into compliance (regardless of methodology or appropriate evidence).
11. There is a need for the broader acceptance of multiple solutions and approaches to guidelines based on common non-specific evidence. Otherwise guidelines and opinion are presumptively rules with some basis in law. Logically, if no responsibility is accepted then there can be no objection to a contrary opinion that relies on the same available evidence. The elevation of LOE IV to evidence requiring an unjustifiable burden of proof would result in in the situation we see in this example.
Conclusion
Whilst the ARC (using the UK and ILCOR practices in ALS), has structured ALS in Australia to be an effective area of emergency management, the same cannot be said for BLS. The level of immediate care (driven by largely hospital-based clinicians) has been weakened by a flawed methodology and process in the use of its own expert consensus opinion. Unlike in higher levels of care, involving clinical professionals, there is no accountability or meaningful scrutiny for decisions made as a result of expert opinion on BLS.
The use of LOE IV should be approached with caution and should be recognised as the lowest form of “evidence” on any hierarchy. There are several pitfalls we see in the methodology when LOE IV – (expert consensus opinion) is used as a substitution for higher levels of evidence, even if influenced in part by stronger evidence. LOE IV cannot be protected by a requirement for higher level of evidence as it is the subjective, momentary interpretation. Protecting this interpretation is weak methodology and impedes innovation and the pursuit of excellence. Ethical and transparent processes must be in place in all considerations of research and evidence, especially when developing widely circulated guidelines. In the absence of proper processes, bias and personal opinion can easily influence group opinion and tends to be self-protective by establishing an unquestionable position. Due to its heavy reliance on LOE IV, the ARC is a good example of the where this methodology can result in sub-optimal guidelines and therefore outcomes in resuscitation. With no accountability for poor methodology and/or the application of the expert opinion and no effective external review together with the assumption of absolute authority in opinion; the example of the ARC demonstrates where evidence methodology can be used as a barrier to genuine consensus and best practice. The question of accountability has still not been resolved and needs to be addressed with a more formal and rigorous approach. Obviating responsibility for outcomes in application at one level is appropriate i.e. as there are no guarantees in any situation that any measure will result in a positive outcome. However, where the recommendation itself is flawed and/or constitutes disparate expert opinion, responsibility must be address, formally acknowledged and be supported by appropriate quality improvement systems to quickly address identified issues.
A discussion, using the example of the Australian Resuscitation Council (ARC) in the formulation of recommendations and guidelines relating to resuscitation.
Author: S. Gould 2016
Aim
The purpose of the paper is to discuss the issues resulting from the use and reliance on expert consensus opinion (referred to in Australian Resuscitation Council or ARC literature as Level of Evidence IV or LOE IV). Further this paper will discuss errors in methodology and interpretation that may and do result in, less than ideal, recommendations in resuscitation practice, especially at BLS level; recommendations that are then implemented verbatim by the end-user, in the mistaken belief that they all represent “best-practice”. This can result in a lack of innovation and a stagnancy or degradation in positive outcomes, without appropriate accountability.
Background
The Australian Resuscitation Council (ARC) is an independent, private, voluntary, non-profit organisation that has representative members from key resuscitation related organisations. These members use a methodology that includes a reliance on Level of Evidence IV – Expert Consensus Opinion (both internally from the International Liaison committee on Resuscitation - ILCOR). While some of this expert opinion in harmonious, some is out of step with current international practice and expert opinion. The constitution of the organisation states that no responsibility is taken for any harm caused by the use of the consensus guidelines and that any recommendation does not mean that any other techniques are ineffective.
ARC LOE IV consensus opinion comes from at least two sources derived from international experts and LOE IV based on a re-analysis by local experts based on a local interpretation of the evidence. These two positions may be substantially different and may be contradictory but are presented as being equally rigorous in their position. This raises an important question about the status and methodology in the formulation of a consensus recommendation based on opinion and how two rigorous methodologies can result in differing end-points. For the individual or group seeking the best advice on which to base their guidelines this situation can be confusing, anomalous and illogical. Classes of LOE IV reflect degrees of confidence in the opinion, but all are presented as “best practice”. The methodology relied upon is that LOE IV is ranked by the evidence influence and therefore is of varying veracity. In actuality, the outcome is the same i.e. it is still a somewhat subjective opinion based on a review of selective research, including the decision to include or reject evidence and the personal opinions of those that make up the expert group. Therefore the LOE IV cannot take on the rigour of the considered evidence. In circumstances where the evidence is weaker the subjectivity increases and the associated rigour and veracity decreases. This variation at the end-user/implementer level is not distinguishable and one would naturally assume that all recommendations are equal in rigour.
Underlying expert consensus opinion using a specific methodology there must be to innate belief that anyone using the same methodology would arrive at the same recommendation. In a general sense this is what one should expect. Whilst this may be true where there is a wide variety of high level research and evidence, the same cannot be said at the other end of the continuum where evidence is weak or inconclusive and where a range of recommendations may reflect and suitably address the evidence. The assumption that is therefore made is that to reach any other conclusion is not scientific and therefore cannot contain any intrinsic value and therefore cannot and will not be considered. This flaw, based in attitude and belief in infallibility of process/ judgement/ methodology is central to much of the latency in the ARC BLS recommendations.
Discussion
Much of resuscitation practices (particularly BLS), have very little targeted and definitive research and so recommendations are determined (for the large part) on low, poor, weak or no direct evidence. Rarely is there such overwhelming strong evidence that one approach is clearly to be used at the exclusion of all others. In this vacuum LOE IV (expert consensus opinion) is used as a substitution and/or a subjective opinion of the conflicting evidence. However, an error in methodology occurs when change or alternate opinion is raised, in that those providing the consensus opinion (LOE IV) now consider that in order to alter their position there is a requirement for strong evidence (i.e. higher than LOE IV). This flaw in process now means that LOE IV has been inappropriately elevated in the evidence hierarchy to an unjustified superior position, presumably based on the level of evidence used to influence the opinion. However, even if influenced by higher levels of evidence i.e. based on strong evidence, as LOE IV it still only represents a subjective interpretation, at a point in time, it cannot assume the status of the underlying influence. It also means that the power of veto in consideration of any evidence is apportioned to the creators of the LOE IV (consensus opinion). This does seem on any level to be a significant flaw in the use of research methodology. Expert opinion can in some instances, be based on, the “discussion” section of a research paper rather than originating from the “conclusion” section, however both are not equal as evidence. Long periods between reviews can also confound the ability of opinion to keep pace/ consider the outcomes from changes in practice recommendations. In fact, proof of efficacy in practice is rarely (if ever) considered or studied as part of this methodology as proof and is not considered necessary and until studied at a formal/ high level (e.g. RCT) it is not taken into account. The history of resuscitation practice is littered with techniques based on expert opinion based on “studies” that were obviously ineffective (and sometimes dangerous) long before expert opinion was changed. As one observer rightly pointed out there are no RCT’s to support the use of parachutes when jumping from a plane and therefore we are totally reliant on informal observation to confirm the benefit over not using a parachute.
In reality, LOE IV is only a substitute for a collection of other evidence (weak and strong) that can be interpreted and/or result in opinion-based implementation strategies. It has little intrinsic merit over any other opinion or approach resulting from a consideration of the available evidence.
LOE IV “evidence” is not at this level in all research hierarchies. For example if we look at Joanna Briggs Institute Levels of Evidence, http://joannabriggs.org/assets/docs/approach/JBI-Levels-of- evidence_2014.pdf we see that consensus opinion by a single expert or a group of experts appropriately sits at Level 5 in the hierarchy i.e. the lowest level, sitting behind any other evidence levels. Likewise in the realms of Level 5 evidence it is only the self-assessed status of those who provide the opinion that guides those seeking direction. Regardless of the source of influence of the consensus opinion, it does not change its position in the hierarchy.
A confounding issue resulting from this self-assessed “expert” status (used in the formulation of consensus view) is each “expert group” can and does claim its own consensus opinion as an absolute and fundamental truth and tends to defend the ownership of this opinion against any contrary observation or ideas that threaten the authority and status perceived to be ascribed to self-assessed “expert opinion”. This is, of course, is not true of all expert groups, however it is certainly the case in Australia. Although this behaviour can and is frequently denied, actions are a better test of character. The close observer will see as a result, contradictory actions and statements that result from this duplicity of motivation. An example from our ARC example is the organisational slogan “Any attempt at resuscitation is better than no resuscitation”. This statement would appear to encourage an individual (particularly the un-trained bystander) to utilise any means they believe is appropriate in an attempt to save a life i.e. “at least one is trying”. The reality of the meaning of this statement is somewhat different and is clearly demonstrated in defensive actions when alternate recommendations are suggested. The actual meaning is “Any resuscitation that follows the ARC recommendations, including its own expert consensus opinion should be attempted; if unable then no resuscitation is better”. This contradiction in statement vs attitude is only supported by the flawed LOE IV status interpretation which we are discussing in this document. Interestingly, the disclaimer used on each recommendation obviates any responsibility for harm or failure of the recommendations to provide the expected outcome and recognises other methods may be of equal or better efficacy. These two statements are essentially and fundamentally contradictory.
The second statement made by the ARC is a disclaimer to the effect that they (the ARC) are not saying that there recommendations are relevant for all circumstances and that individuals should seek “specific advice” in deciding on methods that are applicable to their specific circumstances. Logically, this “specific advice” cannot be from the ARC as it has already (by this statement) referred readers away from the guidelines for advice. Therefore, presumably the statement refers to other sources and/or one’s own review of evidence and recommendations i.e. opinion of relevance. So why do we see such a strong defense of ARC consensus opinion if readers are encouraged to form an opinion independently of the ARC? This statement vs action is also illogical and contradictory in the defense of low level of evidence and demonstrates a misuse of expert opinion.
The other weakness of dogma in local, consensus opinion based recommendations is that the individual agenda of those constituting the expert group can more easily become part of the consensus without the need for the same rigour expected of external potential contributors to the collective opinion. Let us review an example that has been in question for more than a decade. The example from ARC literature is contained in Section 4 – Airway, where recommendations are listed for the management of upper airway obstruction (UAO). Of particular interest is the specific management of an upper airway obstruction (UAO) in the conscious patient. Firstly let us paraphrase the consensus opinion of the ARC and compare this with that of ILCOR and the international resuscitation expert community which includes bodies such as the ERC and AHA.
1. ARC – measures for the relief of UAO include firstly back blows and then “chest thrusts” followed by CPR if unconscious. The recommendation excludes the use of abdominal thrusts and refers to a small, single, yet unrelated postmortem study comparing CPR in a supine position with abdominal thrusts in a living patient.
2. The international resuscitation community – measures for the relief of UAO include firstly back blows and then chest and/or abdominal thrusts, followed by CPR if unconscious. Abdominal thrusts are considered to the most effective technique after the failure of back blows.
Before examining how consensus opinion can have these fundamental differences it is important to note that “chest thrusts” as mentioned in both consensus statements are not equivalent. The technique described by the international resuscitation community is a modified abdominal thrust method suitable when a patient is too large (including pregnancy) to attempt abdominal thrusts. The technique is performed standing behind and against the back of the patient and using two hands pulling toward the centre of the patient’s chest. This technique, as with abdominal thrusts, is supported by respiratory studies that show pressure changes induced in the airway as a result of utilising this technique. Whereas, the “chest thrusts” as described in ARC literature is a modified, single-handed CPR compression technique, that has no supporting respiratory studies or clinical trials.
In terms of our discussion around the use of LOE IV evidence, how did we get to this position that has resulted in a differing recommendation from not only the international resuscitation community, but practice across the world and more importantly after more than a decade no documented cases of success i.e. proof of efficacy. There are several factors that have contributed to this disparate, flawed and unchangeable position.
The ability of expert opinion (LOE IV) to be the re-interpreted by other expert opinion without a need for stronger evidence to support a different outcome. A test consensus opinion does not have to achieve.
The inappropriate direct substitution of unlike terms (such as “chest thrusts) to support a personal view/ opinion and thus take advantage of the outcome and reputation of evidence relating to the original technique without the need to support (with evidence) a experimental method.
The positioning of LOE IV evidence in an artificially elevated position so that strong evidence is required for change, even though the consensus opinion is based on weak, no or poor evidence or borrows rigour from an unrelated finding. This is true regardless of the source influence.
A deliberate dismissal of abdominal thrusts, based on an incomplete consideration of the evidence and a disproportionate emphasis on a misrepresented an “unacceptable risk” (a risk mitigated appropriately and considered against benefit by the international resuscitation community, including ILCOR). The only reason for this position therefore has to come primarily from a personal view of the experts that have contributed to the local expert opinion.
The vehement defense against alternative, (but equally or better evidenced) alternative opinions on the basis that LOE IV evidence has a status above its logical and justified level in research methodology.
A lack of an experimental framework and associated methodology when recommendations are clearly speculative.
What is the result of this difference in consensus opinion? Does it make a difference at the end-user level i.e. to the patient? And what feedback loops are in place to provide proof that one opinion turned out to be better than another? If we review the case of UAO as an example of a divergent view by experts on measures to address the same problem we can see the issues. In Australia an experimental modified chest compression technique and in the rest of the world abdominal thrusts and/or modified abdominal thrust on the chest. Since its inception in 1974 abdominal thrusts in the US have been credited anecdotally by the Washington Post with more than 100,000 saves, whilst in Australia after more than a decade using a different regime there are no documented cases of success. In the recent example in Western Australia a 2 ½ year old child who died after choking on a bubble gum ball he found in his stroller. This was a tragic outcome for the family and those involved and it is uncertain if any measures on the day would have relieved this obstruction. However, what is clear is that in compliance with local expert consensus opinion, 3 separate rescuers (these included a pharmacist, St John Ambulance Volunteers and St Ambulance – State Ambulance) were restricted from using abdominal thrusts and were only able to utilise an experimental technique with little if any supporting evidence (in either clinical trials or field application). The question that should be addressed first is to where in an “all care and no responsibility” methodology does responsibility for review lie. It is doubtful that (unlike an organisation in the general health sector ) that an ARC review (or RCA) of the circumstance has or will take place or seen as necessary in accountability. Differences in recommendations are not restricted to UAO and we see high level guidelines (like BLS Resuscitation) remaining to be focused on a sentimental but uncommon form and cardiac arrest i.e. the hypoxic arrest. This strategic direction, protected by an assumed rigorous methodology, cannot demonstrate improvements in outcome over SCA centered BLS guidelines but cannot be challenged.
Finally, there may be another reason why expert opinion can be at odds with “best practice” or other expert opinion and this relates to ideological and political pressures being brought to bear in the process. Political pressure can arise from dependent organisations, which have an interest in resisting change and the associated costs and imposition of implementing change i.e. the opinion to change can be delayed or moderated as a compromise. Ideological pressures can come from an unwillingness to “confuse” a long term message with change. This assumes that the lowest common denominator (e.g. BLS) is incapable of grasping a new focus or deciding between management options in an emergency. Whilst these pressures can be real considerations in recommendation and guideline development they only gain a controlling power at the LOE IV level where they can build legacy characteristics into recommendations and support sub-optimal guidelines.
Recommendations
The reality in the field of resuscitation is that as we learn more, there will always be better methods being developed than the accepted status quo. They can represent equal levels of opinion and evidence base. The misapplication and defense of any low ranked LOE IV can significantly hamper progress and innovation in guideline development. More significantly it can lead to an unfortunate regression in positive outcomes, when this flawed research methodology is used in resuscitation practice. Recommendation for improvement can be summarised as follows:
1. The adoption of a more appropriate evidence hierarchy system e.g. JBI - Levels of Evidence would more appropriately relegates and classifies consensus opinion. Additionally, nomenclature must clearly differentiate between opinion status and experimental recommendations.
2. Bodies utilising an evidence hierarchy as the basis for any recommendations must exercise appropriate diligence in ensure individual opinion does not unduly affect the consensus view.
3. Ethical and procedural practices need to demonstrate the appropriate and honest representation of research and evidence. The practice of “stolen rigour” used to substitute evidence from unrelated sources must cease immediately, to ensure the maintenance of reputation of expert panels.
4. All consensus opinion based guidelines must be appropriately open to general external scrutiny and peer review and an opportunity for input into development; at any time during the revision cycle. Consultation and comment must represent more than nominal achievements but an important and necessary pathway to excellence.
5. Effective and transparent mechanisms need to be in place to ensure ethical and scientific principles are central to process i.e. that processes are not inappropriately biased toward or away from recommendations for other reasons than a “balance of evidence”.
6. Internal policies that attribute inappropriate status to expert consensus opinion i.e. demand unnecessarily high levels of evidence to affect change; are unscientific and impediments to innovation and improvement.
7. The implementation of an experimental framework and methodology to appropriately manage speculative opinion based recommendations. This framework must necessarily include processes for the evaluation of efficacy to inform change, termination or progression. The use of LOE IV rather than an experimental methodology cannot obviate all responsibility. An experimental framework could allow for the appropriate assessment of regimes or procedures that are currently experimental in nature (due to being significantly different to international consensus opinion) and provide a platform for innovation in the area of resuscitation.
8. Expert consensus opinion should be constructed in consultation with a wider and sector specific group rather than cascading down from higher clinical levels under the assumption that there is an innate understanding of lower levels and their specific implementation/ interpretation challenges. This assumes expert status by inference rather than direct and relevant experience.
9. Any defense of consensus opinion should be done through appropriate debate and dialogue. Strategies such as “refusal to engage” and the “discrediting of individuals” are not appropriate strategies in the consideration of research/ evidence and the formulation of widely utilised guidelines and demonstrate a dedication to power rather than outcome.
10. Those assuming responsibility for guideline development (particularly those based on local consensus opinion) must accept some level of responsibility for the monitoring of efficacy, particularly if unwilling to commit to continuous development. Specifically, if an instrument assumes or has claim as “the authority” which results in others being forced into compliance (regardless of methodology or appropriate evidence).
11. There is a need for the broader acceptance of multiple solutions and approaches to guidelines based on common non-specific evidence. Otherwise guidelines and opinion are presumptively rules with some basis in law. Logically, if no responsibility is accepted then there can be no objection to a contrary opinion that relies on the same available evidence. The elevation of LOE IV to evidence requiring an unjustifiable burden of proof would result in in the situation we see in this example.
Conclusion
Whilst the ARC (using the UK and ILCOR practices in ALS), has structured ALS in Australia to be an effective area of emergency management, the same cannot be said for BLS. The level of immediate care (driven by largely hospital-based clinicians) has been weakened by a flawed methodology and process in the use of its own expert consensus opinion. Unlike in higher levels of care, involving clinical professionals, there is no accountability or meaningful scrutiny for decisions made as a result of expert opinion on BLS.
The use of LOE IV should be approached with caution and should be recognised as the lowest form of “evidence” on any hierarchy. There are several pitfalls we see in the methodology when LOE IV – (expert consensus opinion) is used as a substitution for higher levels of evidence, even if influenced in part by stronger evidence. LOE IV cannot be protected by a requirement for higher level of evidence as it is the subjective, momentary interpretation. Protecting this interpretation is weak methodology and impedes innovation and the pursuit of excellence. Ethical and transparent processes must be in place in all considerations of research and evidence, especially when developing widely circulated guidelines. In the absence of proper processes, bias and personal opinion can easily influence group opinion and tends to be self-protective by establishing an unquestionable position. Due to its heavy reliance on LOE IV, the ARC is a good example of the where this methodology can result in sub-optimal guidelines and therefore outcomes in resuscitation. With no accountability for poor methodology and/or the application of the expert opinion and no effective external review together with the assumption of absolute authority in opinion; the example of the ARC demonstrates where evidence methodology can be used as a barrier to genuine consensus and best practice. The question of accountability has still not been resolved and needs to be addressed with a more formal and rigorous approach. Obviating responsibility for outcomes in application at one level is appropriate i.e. as there are no guarantees in any situation that any measure will result in a positive outcome. However, where the recommendation itself is flawed and/or constitutes disparate expert opinion, responsibility must be address, formally acknowledged and be supported by appropriate quality improvement systems to quickly address identified issues.
The Evidence For and Against Evidence-Based Practice
Edward J. Mullen, DSW, MSW and David L. Streiner, PhD
Edward J. Mullen, DSW, MSW and David L. Streiner, PhD
Review of 2016 ARC Guidelines - the errors, contradictions and missed opportunities
Overall, there is not a lot of positives with the new 2016 ARC Guidelines. Some changes, little improvement, the repetition of traditional, out-dated consensus views and the removal of some key procedures based on a narrow, hospital/physician-centric view of the care of casualties i.e. when a casualty ends up in a hospital with a team of clinical staff to care for them, with a list of invasive and definitive procedures to choose from, the care of the first aider can seem irrelevant and not contributing to any positive outcome. There are also some recommendations that have changed based on the notion that first-aiders are incapable of learning a technique properly and so, “the baby is thrown out with the bath water”.
Provided in the following, is a summary of the issues with these new guidelines for your consideration.
Guideline 3 - Recognition and First Aid Management of the Unconscious Victim
The ARC appropriately defines unconsciousness as… “Unconsciousness is a state of unrousable, unresponsiveness, where the person is unaware of their surroundings and no purposeful response can be obtained.” However, the obvious omission here is the absence of “pain” as the ultimate determinate of “response” and therefore consciousness vs unconsciousness. This omission is carried over into the “Head Injury” guideline were assessment of deteriorating consciousness via GCS or AVPU are not supported for the first aider to use “pain” as a determinate (even in suspected cardiac arrest) of unconsciousness. “Pain” as a clinical indicator is safely used everywhere in the management and assessment of casualties and patients, except in these BLS guidelines for first aiders. The ARC continues to rely on the assessment of consciousness as accurately determinable by “gentle shaking of the shoulders and talking to the casualty”, even in determining suspected cardiac arrest. This is neither effective nor clinically sound.
Guideline 4 – Airway
In this guideline the ARC makes several contradictory and confusing statements that are not supported by evidence and have remained uncorrected.
1 “To clear the airway the mouth should be opened and the head turned slightly downwards to allow any obvious foreign material (e.g. food, vomit, blood and secretions) to drain.”
This technique 1 is contradictory to 2 below. 1 uses a technique that (as the casualty is supine) will not make a scrap of difference in “clearing the airway”. However the technique in 2 “if the airway is obstructed” is the exception for log rolling a casualty.
“The person should not be routinely rolled onto the side to assess airway and breathing—leave them in the position in which they have been found. This has the advantages of simplified teaching, taking less time to perform and avoids movement.
2"The exceptions to this would be where the airway is obstructed with fluid (water or blood) or matter (sand, debris, vomit). Here, the person should be promptly rolled onto their side to clear the airway.”
The other continuing error here is that log rolling for “debris” may be of limited value. However, the only fluid that makes a difference to outcome in resuscitation is vomitus in the airway i.e. the only indication to log-roll is therefore vomit. Blood is rarely present in sufficient quantities to create issues, water (salt or fresh) rarely causes significant issues (e.g. delayed pulmonary oedema), and secretions are not a significant issue and like most fluids will disappear across the lung tissue with ventilation.
Later in this guideline we come across the statement by the ARC in relation to FBAO in the conscious casualty i.e. “If back blows are unsuccessful the rescuer should perform up to five chest thrusts. To perform chest thrusts, identify the same compression point as for CPR and give up to five chest thrusts. These are similar to chest compressions but sharper and delivered at a slower rate.”
In response to this it must be reiterated that the “chest thrust” technique recommended here by the ARC has no clinical evidence, trials, and respiratory studies, nor survivors and is not the “chest thrusts” described in the international literature; or the recommended treatment by ILCOR after the failure of back blows i.e. abdominal thrusts.
Guideline 5 - Breathing
Here in this guideline there is a mixture of terms. The term “rescue breathing” is used as before, however the proper term for this process is also mentioned i.e. “ventilation”. The term “rescue breathing” is a left-over from the EAR days when the only VENTILATION of a patient was done with one’s mouth.
In the “Mouth to Nose” section the ARC has recommended that this technique be used:
• “where the rescuer chooses to do so”
• “where the person’s jaws are tightly clenched”
• “when resuscitating infants and small children”
However in practice, this technique (when used in cases of hypoxic arrest) is most useful when:
The fact that “No human studies have addressed the safety, effectiveness, or feasibility of using barrier devices to prevent person-to-rescuer contact during rescuer breathing” does not mean this method should not be preferred over direct contact.
The new statement that “ANZCOR suggests that those who are trained and willing to give breaths do so for all persons who are unresponsive and not breathing normally” is not supported by the findings of the 2010 ILCOR in that “In some circumstances the inclusion of ventilations in resuscitation attempts, led to poorer outcomes”. This reduction in poorer outcome was put down to poor technique (poor airway care and hyperventilation – leading to aspiration) and wasting time in SCA where passive ventilation via compressions was considered adequate in BLS for SCA.
Guideline 6 - Compressions
The assumption made in this guideline is that all cardiac arrests happen with more than one rescuer present, that all rescuers are capable of providing adequate chest compressions using a kneeling technique and that there is only one method of effecting compressions. In reality approximately 46% of the adult population (including health professionals) are able to achieve adequate depth of compression on an adult casualty using the kneeling technique. The statement that “ANZCOR suggests performing chest compressions on the lower half of the sternum. In making this recommendation, we place a high value on consistency with current treatment recommendations in the absence of compelling data suggesting the need to change the recommended approach. Place the heel of their hand in the centre of the chest with the other hand on top.” This statement merely means that the ARC has formed an opinion based on internal consensus rather than evidence contrary to their view. Other techniques, including “pedal compressions” are more effective for rescuers with low strength and/or body mass or those with an injury or disability and who have no assistance available. Pedal compressions are the only method in fact that can maintain depth of compressions after the first few minutes.
The next section of the guidelines in relation to depth and rate seems to make little sense and is full of questionable statements that are in opposition to the international evidence and common sense.
“The lower half of the sternum should be depressed approximately Œone third of the depth of the chest with each compression. This equates to more than 5cm in adults, approximately 5cm in children and 4 cm in infants. ANZCOR places greater importance on adequate compression depth. Although there is some evidence suggesting detriment with compression depths greater than 6cm, the clinical reality of being able to tell the difference between 5 or 6 cm and adjust compressions accordingly is questionable. Inadequate compression depth is definitely associated with poor outcomes. ANZCOR has elected not to put an upper limit on compression depth as the risk of too shallow compressions outweighs the risk of compressions that are too deep. “
The concept of every casualty being compressed approximately 1/3 of the depth of the chest is an ARCism that in the adult casualty is anatomically impossible. The typical chest depth achieved by compressions on an adult is in the order of 20% and so this assertion is incorrect. Additionally, how in practice would a sole rescuer determine a fraction of 1/3 from a position over the casualty?! The measurements used re-enforce the error of 1/3. The suggested depth on an adult and child here the same (5cm). Whilst 5cm in children and 4 centimetres in infants do represent approximately 1/3 of the chest depth, anatomically the adult approximation must be wrong or a 3 year old has the same chest depth as a 40 year old. As the ARC acknowledges the 6cm depth (used in the UK and Europe for some time), it suggested that a rationale for not increasing their recommendation (which we have established is wrong) is that the new depth would be impossible to estimate. As stated 1/3 in adults is not only wrong anatomically, but is impossible also to determine by the sole rescuer. The risk to casualties of too shallow compressions is vastly understated. Except in the very old and frail, the main failure of adequate compressions comes from too shallow compressions rather than too deep compressions. This is not therefore a rationale for not applying an upper limit.
Later in the revision, the statement on rate below is inserted into the new guidelines:
“ANZCOR acknowledges that compression rates will vary between and within providers and survival rates are optimised at compressions rates of 100-120 compressions per minute. There is some evidence that compressions rates less than 100 or greater than 140 compressions per minute are associated with lower rates of survival.”
Here again we see an acknowledgement that international practice has evidence of improved outcomes with a faster rate, but the ARC fails to provide clear guidance around an optimum value i.e. 120 /min. An aspirational goal would have been helpful here as an appropriate benchmark.
Later in the guideline the ARC makes another interesting statement in relation to CPR feedback devices (presumably including those within AED’s) that is contradictory to its own methodology:
“There is no high level evidence that the use of CPR feedback devices during real time CPR improves survival or return of spontaneous circulation. CPR prompt / feedback devices may be considered for clinical use to provide data as part of an overall strategy to improve quality of CPR at a systems level. ANZCOR places a higher value on resource allocation and cost effectiveness than widespread implementation of a technology with uncertain effectiveness during real time CPR. We acknowledge that data provided by CPR feedback devices may benefit other victims as part of a broader quality improvement system.”
The absence of “high level evidence” in relation to recommendations made by the ARC is not a pre-requisite for exclusion. There are many techniques recommended by the ARC that are made on low, no or very poor levels of evidence. Feedback devices, especially when used by individuals with little or no real exposure to resuscitation, just make good sense. The question to the ARC from the statement above is if “CPR prompt / feedback devices may be considered for clinical use to provide data as part of an overall strategy to improve quality of CPR at a systems level.” what is the difference for improving systems at the first responder level? The data is real time and does not need clinical/ academic review to prompt immediate improvement.
Lastly in this guideline is a welcome but again contradictory statement:
“Rib fractures and other injuries are common but acceptable consequences of CPR given the alternative of death. CPR should be initiated for presumed cardiac arrest without concerns of harm to patients not in cardiac arrest. In making this recommendation, ANZCOR places a higher value on the survival benefit of CPR initiated by laypersons for patients in cardiac arrest against the low risk of injury in patients not in cardiac arrest.”
Whilst this statement is absolutely true and refreshing, the theory is not universally applied to examples such as FBAO when the consequence of non-relief is death.
Guideline 7 – External Automated Defibrillation in BLS
This guideline sets out the recommendations in relation to the use of AEDs, however the there is a lack of detail in the following leading to an obvious interpretation by some who read and implement this guideline.
“If the AED does not have a paediatric mode or paediatric pads then it is reasonable to proceed with standard adult AED pads.”
This would suggest that it is acceptable to not purchase a defibrillator with a paediatric switch or purchase paediatric pads, because adult pads can be routinely substituted. The recommendation should read “In cases of emergency, where the AED available is not fitted with a paediatric switch or paediatric pads, the adult pads can be used. The substitution of adult pads for paediatric pads is not a recommended strategy for the management of casualties in cardiac arrest. ANZCOR recommends that the type of defibrillator available and the pads stored in the machine should reflect the risk associated with the AED’s location and intended use.”
9.1.1 – Principle of Controlling Bleeding for First Aiders.
This guideline’s recommendation changes are a little puzzling. Whilst there may be no evidence that elevation of a bleeding part will control severe bleeding, it is extremely doubtful that there is no evidence that as a self-care measure, for instance, in the management of minor bleeding that this technique is effective. This is also true for pressure points.
“There is no evidence that elevation of a bleeding part aids control of bleeding and there is the potential to cause more pain or injury.”
Certainly in the face of severe or life-threatening haemorrhage, elevation may have little use, however the “potential to cause more pain and injury” is far more from tourniquets and the like, so this rationale is not particularly valid. This guideline change assumes that all bleeding is haemorrhagic and severe.
9.1.4 Head Injury
The head injury guideline unfortunately makes no distinction between, for example, a facial laceration/bruise and a head (brain injury). The notion that all casualties with wounds to the face or head have a “brain injury” and need to be “assessed” in hospital is not supported by the evidence and is totally unworkable (particularly in sports). This would mean, for example, the first time a boxer was hit in the first seconds of the first round he/she needs to be taken to hospital.
“A brain injury should be suspected if the victim has a reported or witnessed injury, has signs of injury to the head or face such as bruises or bleeding, or is found in a confused or unconscious state. A victim may have a brain injury without external signs of injury to the head or face. Serious problems may not be obvious for several hours after the initial injury.”
Undetected brain injuries are not common and can occur even after assessment in a hospital. It would be expected that considering the resource implications of such a recommendation, this would be supported by a high level of evidence. Whilst the Glasgow Coma Score is not well understood or implemented by first aiders (particularly when faced with a young child or mute), and should not be used as an absolute determinate of head injury; surely any altered LOC at or after an injury (or a high risk event), is a stronger indication of concern requiring hospitalisation.
There is also no mention in this guideline of the higher likelihood of a neck injury with brain injury.
9.1.6 Spinal Injury
Of the guideline changes, the changes to this guideline are obviously the recommendation of hospital-based trauma physicians with little appreciation for the circumstances and challenges faced by first-aiders. There is also a failure in this guideline to take the opportunity to improve the techniques and methods of spinal care pre-hospital and provide what is actually missing from the SR Cervical collar debate, standards for proper training in the effective application of collars and improved methods. The statement in the new guidelines below appears to be little more than an opinion based on, at best, anecdotal evidence of the authors.
“The use of SR (cervical collars) by first aid providers is not recommended.” Although this is listed as a weak recommendation with low quality evidence.
The evidences used by the ARC are:
Hauswald M, Hsu M, Stockoff C: Maximizing Comfort and Minimizing Ischemia: A Comparison of Four methods of Spinal Immobilization. Pre-hospital Emergency Care. 2000; 4: 250-252 - which concluded that SR cervical collar application in the pre-hospital setting is prudent and the primary source of morbidity was the transport of victims on hard backboards. It also suggested that additional padding could vastly improve comfort and fitting issues. Some unsupported discussion/speculation in the research has also been used by the ARC as evidence.
Hood N, Considine J: Spinal Immobilisation in Pre-hospital and Emergency Care: A Systematic Review of the Literature. Australasian Emergency Nursing Journal 2015; 18(3):118-137 - which found that there was a balance of fair and poor (no good studies with good quality evidence) studies for and against pre-hospital spinal immobilisation.
"There are no published high-level studies that assess the efficacy of spinal immobilisation in the pre-hospital and emergency care settings. Almost all of the current evidence related to spinal immobilisation is extrapolated data, mostly from healthy volunteers. There were no studies that showed spinal immobilisation improved neurological outcomes as all studies using neurological outcome as an endpoint were neutral due to high mortality rates from other causes (mostly gunshot wounds)...Protocols that recommend application of spinal immobilisation should consider the risk vs benefits. Prospective studies of patients at risk of, or with actual spinal injuries, are needed using real pre-hospital or clinical environments."
It also reinforced that the Canadian C-Spine Rule has 100% sensitivity and 42.5% specificity which should be considered as an indicator for cervical spine immobilisation in the pre-hospital setting (see also Nexus).
Hauswald M, Ong G, Tandberg D, Omar Z: Out-of-hospital Spinal immobilization: Its Effect on Neurologic Injury. Academic Emergency Medicine. 1998; vol5, 3: 214-219 - which did not show a causation, was a relatively small sample and acknowledged that the observation that the non-immobilised group had less neurological injury could have been related to a difference in other more serious associated injuries (which was not part of the research corrections in data).
Zideman, D. A., Singletary, E. M., De Buck, E.,et al. (2015). Part 9: First aid: 2015 International Consensus on First Aid Science with Treatment Recommendations. Resuscitation, 95, e225. -
which acknowledged that "more evidence is needed on manual stabilization (using hands/knees to restrict motion), trauma patients in the pre-hospital setting, high-risk versus low-risk patients, other forms of physical cervical spinal stabilization, and implementation and education. A review of the adverse effects as a consequence of application of a cervical collar could be interesting in the future."
Although not recommending SR cervical collars in first aid, this was based on poor training and the risk criteria used in determining the need for a cervical collar; two elements that could be addressed directly.
The application of SR Cervical Collars is an interim emergency measure until more effective means are available. The suggestion that all the first aider needs to do is to have someone stabilise the head during treatment and transport, again neglects to recognise that the movement, extrication and transport of casualties is often required to meet emergency services or remove them from danger and that not all first aiders will have a team around them (as in an ED) to be able to sacrifice one person to “look after the stabilisation of the head and neck”.
The rationale that unnecessary movement is caused by the “sizing and fitting of collars” and that other complications “may” occur (including increased intra-cranial pressure) just means that some direction may be helpful for the proper training in the safe fitting and sizing of collars (a task that many clinicians do not understand well). This is another example of “the baby out with the bath water”. The other missed opportunity in this guideline is a recommendation around head immobilisation boards with specific padding, as a preferred adjunct rather than the reliance on cervical collars.
9.2.3 Shock
The definition and management of shock by the first aider has always created much confusion in the non-clinical individual. For the most part, without a clear understanding, shock is assumed by the first aider in every emergency and is confused frequently with “emotional distress”. What are lacking in this guideline are changes to clarify the position and assist in determining likelihood and more specific deferential diagnosis.
“For individuals with shock who are in the supine position and with no evidence of trauma, the use of PLR (passive leg raise) may provide a transient (less than 7 minutes) improvement.”
“The clinical significance of this transient improvement is uncertain; however, no study reported adverse effects due to PLR. Because improvement with PLR is brief and its clinical significance uncertain, ANZCOR recommends the supine position without passive leg raising for victims of shock”
The new statements above in the guideline fail to recognise 4 essential factors in the first aid management of patients.
9.2.5 First Aid for Asthma
The new revision for the management of asthma has not corrected a significant failing of the old guideline; in that there is still no trigger for calling an Ambulance without first giving the “up to 6 puffs and wait 4-6 minutes then give another 4-6 puffs”. A casualty in extremis, who is hyper-inflated, will receive no benefit from inhaled broncho-dilators or the accumulated wait time of more than 6 minutes.
There is also no acknowledgement of techniques such as “sustained lateral expiratory chest thrusts” in the management of severe asthma. This technique, in the absence of adrenaline, can mean the difference between a dead asthmatic and a treatable one. This technique has good evidence and has been re-instated in all Ambulance protocols. See Allan, J., Williams, B., & Fallows, B. (2007). Investigating the Benefits of Out-of-Hospital External Chest Compression. Australasian Journal of Paramedicine, 5(3). Retrieved from http://ro.ecu.edu.au/jephc/vol5/iss3/2
10.4 Use of Oxygen in Emergencies
The changes to use of oxygen in emergencies have changed significantly after the research done by the UK Anaesthetics Society several years ago. Australia is now playing a bit of catch up regarding the use of oxygen. Unfortunately, there are some disparities and anomalies in the guidelines between the recommendations for ALS vs BLS. Whilst the ARC is aware of these anomalies, no changes have been made to address these issues. For example, the guideline states:
“When bag-valve-mask oxygen resuscitation is used by trained but occasional operators, a minimum of two trained rescuers are required to provide ventilation for a non-breathing victim.”
However many ALS operators would be considered “occasional” and there is no stipulation that they “are required” to use two operators. Surely the standard should be competence in one person ventilation (after all first aiders do not travel in groups for the most part) and on failure of this, then two-person (if available) delivery.
Conclusion
In reviewing the summary of changes in the 2016 ANZCOR Guidelines, it is apparent to ARAN that they have fallen short of their potential to promote improvement in casualty outcomes and better equip first aiders to provide effective, evidenced-based foundations to their care. The individual guidelines are inconsistent and contradictory in both terminology and the use of evidence on which is based recommendations and consensus view. It is apparent that many authors have controlled the review of individual sections, without a consistent approach to the purpose, implications and evidence required to inform consensus view over scientific literature and clinical findings. This misuse of evidence-based review leads to therapeutic nihilism (the belief that there is no objective basis for truth) in the absence of evidence from randomized trials.
Historically, highlighting issues such as these to the ARC and/or the submission of constructive, evidenced suggestions are met with silence. This is followed by complete dismissal (without explanation, discussion or the provision of counter evidence). This must suggest that to the observer, that the methodology of review and evidence used by the ARC is flawed, partisan and conceited. This unfortunately means that there is no current, effective means of influencing change in the ARC published guidelines in Australia regardless of one’s evidence and/or clinical standing (outside of its internal structure) and thus no peer review.
ARAN suggests that individuals (both clinical and non-clinical) closely review the new ANZCOR guidelines for themselves to determine their consistency and efficacy and then independently decide if the ARC Guidelines (opinions as published) are suitable and relevant for their individual situation.
Provided in the following, is a summary of the issues with these new guidelines for your consideration.
Guideline 3 - Recognition and First Aid Management of the Unconscious Victim
The ARC appropriately defines unconsciousness as… “Unconsciousness is a state of unrousable, unresponsiveness, where the person is unaware of their surroundings and no purposeful response can be obtained.” However, the obvious omission here is the absence of “pain” as the ultimate determinate of “response” and therefore consciousness vs unconsciousness. This omission is carried over into the “Head Injury” guideline were assessment of deteriorating consciousness via GCS or AVPU are not supported for the first aider to use “pain” as a determinate (even in suspected cardiac arrest) of unconsciousness. “Pain” as a clinical indicator is safely used everywhere in the management and assessment of casualties and patients, except in these BLS guidelines for first aiders. The ARC continues to rely on the assessment of consciousness as accurately determinable by “gentle shaking of the shoulders and talking to the casualty”, even in determining suspected cardiac arrest. This is neither effective nor clinically sound.
Guideline 4 – Airway
In this guideline the ARC makes several contradictory and confusing statements that are not supported by evidence and have remained uncorrected.
1 “To clear the airway the mouth should be opened and the head turned slightly downwards to allow any obvious foreign material (e.g. food, vomit, blood and secretions) to drain.”
This technique 1 is contradictory to 2 below. 1 uses a technique that (as the casualty is supine) will not make a scrap of difference in “clearing the airway”. However the technique in 2 “if the airway is obstructed” is the exception for log rolling a casualty.
“The person should not be routinely rolled onto the side to assess airway and breathing—leave them in the position in which they have been found. This has the advantages of simplified teaching, taking less time to perform and avoids movement.
2"The exceptions to this would be where the airway is obstructed with fluid (water or blood) or matter (sand, debris, vomit). Here, the person should be promptly rolled onto their side to clear the airway.”
The other continuing error here is that log rolling for “debris” may be of limited value. However, the only fluid that makes a difference to outcome in resuscitation is vomitus in the airway i.e. the only indication to log-roll is therefore vomit. Blood is rarely present in sufficient quantities to create issues, water (salt or fresh) rarely causes significant issues (e.g. delayed pulmonary oedema), and secretions are not a significant issue and like most fluids will disappear across the lung tissue with ventilation.
Later in this guideline we come across the statement by the ARC in relation to FBAO in the conscious casualty i.e. “If back blows are unsuccessful the rescuer should perform up to five chest thrusts. To perform chest thrusts, identify the same compression point as for CPR and give up to five chest thrusts. These are similar to chest compressions but sharper and delivered at a slower rate.”
In response to this it must be reiterated that the “chest thrust” technique recommended here by the ARC has no clinical evidence, trials, and respiratory studies, nor survivors and is not the “chest thrusts” described in the international literature; or the recommended treatment by ILCOR after the failure of back blows i.e. abdominal thrusts.
Guideline 5 - Breathing
Here in this guideline there is a mixture of terms. The term “rescue breathing” is used as before, however the proper term for this process is also mentioned i.e. “ventilation”. The term “rescue breathing” is a left-over from the EAR days when the only VENTILATION of a patient was done with one’s mouth.
In the “Mouth to Nose” section the ARC has recommended that this technique be used:
• “where the rescuer chooses to do so”
• “where the person’s jaws are tightly clenched”
• “when resuscitating infants and small children”
However in practice, this technique (when used in cases of hypoxic arrest) is most useful when:
- The casualty has a large mouth i.e. smaller rescuer
- The casualty has no teeth
The fact that “No human studies have addressed the safety, effectiveness, or feasibility of using barrier devices to prevent person-to-rescuer contact during rescuer breathing” does not mean this method should not be preferred over direct contact.
The new statement that “ANZCOR suggests that those who are trained and willing to give breaths do so for all persons who are unresponsive and not breathing normally” is not supported by the findings of the 2010 ILCOR in that “In some circumstances the inclusion of ventilations in resuscitation attempts, led to poorer outcomes”. This reduction in poorer outcome was put down to poor technique (poor airway care and hyperventilation – leading to aspiration) and wasting time in SCA where passive ventilation via compressions was considered adequate in BLS for SCA.
Guideline 6 - Compressions
The assumption made in this guideline is that all cardiac arrests happen with more than one rescuer present, that all rescuers are capable of providing adequate chest compressions using a kneeling technique and that there is only one method of effecting compressions. In reality approximately 46% of the adult population (including health professionals) are able to achieve adequate depth of compression on an adult casualty using the kneeling technique. The statement that “ANZCOR suggests performing chest compressions on the lower half of the sternum. In making this recommendation, we place a high value on consistency with current treatment recommendations in the absence of compelling data suggesting the need to change the recommended approach. Place the heel of their hand in the centre of the chest with the other hand on top.” This statement merely means that the ARC has formed an opinion based on internal consensus rather than evidence contrary to their view. Other techniques, including “pedal compressions” are more effective for rescuers with low strength and/or body mass or those with an injury or disability and who have no assistance available. Pedal compressions are the only method in fact that can maintain depth of compressions after the first few minutes.
The next section of the guidelines in relation to depth and rate seems to make little sense and is full of questionable statements that are in opposition to the international evidence and common sense.
“The lower half of the sternum should be depressed approximately Œone third of the depth of the chest with each compression. This equates to more than 5cm in adults, approximately 5cm in children and 4 cm in infants. ANZCOR places greater importance on adequate compression depth. Although there is some evidence suggesting detriment with compression depths greater than 6cm, the clinical reality of being able to tell the difference between 5 or 6 cm and adjust compressions accordingly is questionable. Inadequate compression depth is definitely associated with poor outcomes. ANZCOR has elected not to put an upper limit on compression depth as the risk of too shallow compressions outweighs the risk of compressions that are too deep. “
The concept of every casualty being compressed approximately 1/3 of the depth of the chest is an ARCism that in the adult casualty is anatomically impossible. The typical chest depth achieved by compressions on an adult is in the order of 20% and so this assertion is incorrect. Additionally, how in practice would a sole rescuer determine a fraction of 1/3 from a position over the casualty?! The measurements used re-enforce the error of 1/3. The suggested depth on an adult and child here the same (5cm). Whilst 5cm in children and 4 centimetres in infants do represent approximately 1/3 of the chest depth, anatomically the adult approximation must be wrong or a 3 year old has the same chest depth as a 40 year old. As the ARC acknowledges the 6cm depth (used in the UK and Europe for some time), it suggested that a rationale for not increasing their recommendation (which we have established is wrong) is that the new depth would be impossible to estimate. As stated 1/3 in adults is not only wrong anatomically, but is impossible also to determine by the sole rescuer. The risk to casualties of too shallow compressions is vastly understated. Except in the very old and frail, the main failure of adequate compressions comes from too shallow compressions rather than too deep compressions. This is not therefore a rationale for not applying an upper limit.
Later in the revision, the statement on rate below is inserted into the new guidelines:
“ANZCOR acknowledges that compression rates will vary between and within providers and survival rates are optimised at compressions rates of 100-120 compressions per minute. There is some evidence that compressions rates less than 100 or greater than 140 compressions per minute are associated with lower rates of survival.”
Here again we see an acknowledgement that international practice has evidence of improved outcomes with a faster rate, but the ARC fails to provide clear guidance around an optimum value i.e. 120 /min. An aspirational goal would have been helpful here as an appropriate benchmark.
Later in the guideline the ARC makes another interesting statement in relation to CPR feedback devices (presumably including those within AED’s) that is contradictory to its own methodology:
“There is no high level evidence that the use of CPR feedback devices during real time CPR improves survival or return of spontaneous circulation. CPR prompt / feedback devices may be considered for clinical use to provide data as part of an overall strategy to improve quality of CPR at a systems level. ANZCOR places a higher value on resource allocation and cost effectiveness than widespread implementation of a technology with uncertain effectiveness during real time CPR. We acknowledge that data provided by CPR feedback devices may benefit other victims as part of a broader quality improvement system.”
The absence of “high level evidence” in relation to recommendations made by the ARC is not a pre-requisite for exclusion. There are many techniques recommended by the ARC that are made on low, no or very poor levels of evidence. Feedback devices, especially when used by individuals with little or no real exposure to resuscitation, just make good sense. The question to the ARC from the statement above is if “CPR prompt / feedback devices may be considered for clinical use to provide data as part of an overall strategy to improve quality of CPR at a systems level.” what is the difference for improving systems at the first responder level? The data is real time and does not need clinical/ academic review to prompt immediate improvement.
Lastly in this guideline is a welcome but again contradictory statement:
“Rib fractures and other injuries are common but acceptable consequences of CPR given the alternative of death. CPR should be initiated for presumed cardiac arrest without concerns of harm to patients not in cardiac arrest. In making this recommendation, ANZCOR places a higher value on the survival benefit of CPR initiated by laypersons for patients in cardiac arrest against the low risk of injury in patients not in cardiac arrest.”
Whilst this statement is absolutely true and refreshing, the theory is not universally applied to examples such as FBAO when the consequence of non-relief is death.
Guideline 7 – External Automated Defibrillation in BLS
This guideline sets out the recommendations in relation to the use of AEDs, however the there is a lack of detail in the following leading to an obvious interpretation by some who read and implement this guideline.
“If the AED does not have a paediatric mode or paediatric pads then it is reasonable to proceed with standard adult AED pads.”
This would suggest that it is acceptable to not purchase a defibrillator with a paediatric switch or purchase paediatric pads, because adult pads can be routinely substituted. The recommendation should read “In cases of emergency, where the AED available is not fitted with a paediatric switch or paediatric pads, the adult pads can be used. The substitution of adult pads for paediatric pads is not a recommended strategy for the management of casualties in cardiac arrest. ANZCOR recommends that the type of defibrillator available and the pads stored in the machine should reflect the risk associated with the AED’s location and intended use.”
9.1.1 – Principle of Controlling Bleeding for First Aiders.
This guideline’s recommendation changes are a little puzzling. Whilst there may be no evidence that elevation of a bleeding part will control severe bleeding, it is extremely doubtful that there is no evidence that as a self-care measure, for instance, in the management of minor bleeding that this technique is effective. This is also true for pressure points.
“There is no evidence that elevation of a bleeding part aids control of bleeding and there is the potential to cause more pain or injury.”
Certainly in the face of severe or life-threatening haemorrhage, elevation may have little use, however the “potential to cause more pain and injury” is far more from tourniquets and the like, so this rationale is not particularly valid. This guideline change assumes that all bleeding is haemorrhagic and severe.
9.1.4 Head Injury
The head injury guideline unfortunately makes no distinction between, for example, a facial laceration/bruise and a head (brain injury). The notion that all casualties with wounds to the face or head have a “brain injury” and need to be “assessed” in hospital is not supported by the evidence and is totally unworkable (particularly in sports). This would mean, for example, the first time a boxer was hit in the first seconds of the first round he/she needs to be taken to hospital.
“A brain injury should be suspected if the victim has a reported or witnessed injury, has signs of injury to the head or face such as bruises or bleeding, or is found in a confused or unconscious state. A victim may have a brain injury without external signs of injury to the head or face. Serious problems may not be obvious for several hours after the initial injury.”
Undetected brain injuries are not common and can occur even after assessment in a hospital. It would be expected that considering the resource implications of such a recommendation, this would be supported by a high level of evidence. Whilst the Glasgow Coma Score is not well understood or implemented by first aiders (particularly when faced with a young child or mute), and should not be used as an absolute determinate of head injury; surely any altered LOC at or after an injury (or a high risk event), is a stronger indication of concern requiring hospitalisation.
There is also no mention in this guideline of the higher likelihood of a neck injury with brain injury.
9.1.6 Spinal Injury
Of the guideline changes, the changes to this guideline are obviously the recommendation of hospital-based trauma physicians with little appreciation for the circumstances and challenges faced by first-aiders. There is also a failure in this guideline to take the opportunity to improve the techniques and methods of spinal care pre-hospital and provide what is actually missing from the SR Cervical collar debate, standards for proper training in the effective application of collars and improved methods. The statement in the new guidelines below appears to be little more than an opinion based on, at best, anecdotal evidence of the authors.
“The use of SR (cervical collars) by first aid providers is not recommended.” Although this is listed as a weak recommendation with low quality evidence.
The evidences used by the ARC are:
Hauswald M, Hsu M, Stockoff C: Maximizing Comfort and Minimizing Ischemia: A Comparison of Four methods of Spinal Immobilization. Pre-hospital Emergency Care. 2000; 4: 250-252 - which concluded that SR cervical collar application in the pre-hospital setting is prudent and the primary source of morbidity was the transport of victims on hard backboards. It also suggested that additional padding could vastly improve comfort and fitting issues. Some unsupported discussion/speculation in the research has also been used by the ARC as evidence.
Hood N, Considine J: Spinal Immobilisation in Pre-hospital and Emergency Care: A Systematic Review of the Literature. Australasian Emergency Nursing Journal 2015; 18(3):118-137 - which found that there was a balance of fair and poor (no good studies with good quality evidence) studies for and against pre-hospital spinal immobilisation.
"There are no published high-level studies that assess the efficacy of spinal immobilisation in the pre-hospital and emergency care settings. Almost all of the current evidence related to spinal immobilisation is extrapolated data, mostly from healthy volunteers. There were no studies that showed spinal immobilisation improved neurological outcomes as all studies using neurological outcome as an endpoint were neutral due to high mortality rates from other causes (mostly gunshot wounds)...Protocols that recommend application of spinal immobilisation should consider the risk vs benefits. Prospective studies of patients at risk of, or with actual spinal injuries, are needed using real pre-hospital or clinical environments."
It also reinforced that the Canadian C-Spine Rule has 100% sensitivity and 42.5% specificity which should be considered as an indicator for cervical spine immobilisation in the pre-hospital setting (see also Nexus).
Hauswald M, Ong G, Tandberg D, Omar Z: Out-of-hospital Spinal immobilization: Its Effect on Neurologic Injury. Academic Emergency Medicine. 1998; vol5, 3: 214-219 - which did not show a causation, was a relatively small sample and acknowledged that the observation that the non-immobilised group had less neurological injury could have been related to a difference in other more serious associated injuries (which was not part of the research corrections in data).
Zideman, D. A., Singletary, E. M., De Buck, E.,et al. (2015). Part 9: First aid: 2015 International Consensus on First Aid Science with Treatment Recommendations. Resuscitation, 95, e225. -
which acknowledged that "more evidence is needed on manual stabilization (using hands/knees to restrict motion), trauma patients in the pre-hospital setting, high-risk versus low-risk patients, other forms of physical cervical spinal stabilization, and implementation and education. A review of the adverse effects as a consequence of application of a cervical collar could be interesting in the future."
Although not recommending SR cervical collars in first aid, this was based on poor training and the risk criteria used in determining the need for a cervical collar; two elements that could be addressed directly.
The application of SR Cervical Collars is an interim emergency measure until more effective means are available. The suggestion that all the first aider needs to do is to have someone stabilise the head during treatment and transport, again neglects to recognise that the movement, extrication and transport of casualties is often required to meet emergency services or remove them from danger and that not all first aiders will have a team around them (as in an ED) to be able to sacrifice one person to “look after the stabilisation of the head and neck”.
The rationale that unnecessary movement is caused by the “sizing and fitting of collars” and that other complications “may” occur (including increased intra-cranial pressure) just means that some direction may be helpful for the proper training in the safe fitting and sizing of collars (a task that many clinicians do not understand well). This is another example of “the baby out with the bath water”. The other missed opportunity in this guideline is a recommendation around head immobilisation boards with specific padding, as a preferred adjunct rather than the reliance on cervical collars.
9.2.3 Shock
The definition and management of shock by the first aider has always created much confusion in the non-clinical individual. For the most part, without a clear understanding, shock is assumed by the first aider in every emergency and is confused frequently with “emotional distress”. What are lacking in this guideline are changes to clarify the position and assist in determining likelihood and more specific deferential diagnosis.
“For individuals with shock who are in the supine position and with no evidence of trauma, the use of PLR (passive leg raise) may provide a transient (less than 7 minutes) improvement.”
“The clinical significance of this transient improvement is uncertain; however, no study reported adverse effects due to PLR. Because improvement with PLR is brief and its clinical significance uncertain, ANZCOR recommends the supine position without passive leg raising for victims of shock”
The new statements above in the guideline fail to recognise 4 essential factors in the first aid management of patients.
- The guideline assumes that a non-clinician can determine between “shock” and syncope from other causes. PLR is a reasonable differential test for syncope.
- A 7 minute improvement in a true “shock victim” is in fact when the “first aider” is working, that is why they call it “first aid”.
- The first aider does not have access to more definitive means of managing shock than PLR. Certainly compared to plasma expanders PLR may seem ineffective, however in the absence of an alternative, there is also no evidence quoted that it does any harm just 7 minutes of improvement.
- The fact that “no study reported adverse effects due to PLR” is a curious reason to not recommend it. What more evidence is required other that a short term positive effect and no adverse effect? This does not make the “significance uncertain”.
9.2.5 First Aid for Asthma
The new revision for the management of asthma has not corrected a significant failing of the old guideline; in that there is still no trigger for calling an Ambulance without first giving the “up to 6 puffs and wait 4-6 minutes then give another 4-6 puffs”. A casualty in extremis, who is hyper-inflated, will receive no benefit from inhaled broncho-dilators or the accumulated wait time of more than 6 minutes.
There is also no acknowledgement of techniques such as “sustained lateral expiratory chest thrusts” in the management of severe asthma. This technique, in the absence of adrenaline, can mean the difference between a dead asthmatic and a treatable one. This technique has good evidence and has been re-instated in all Ambulance protocols. See Allan, J., Williams, B., & Fallows, B. (2007). Investigating the Benefits of Out-of-Hospital External Chest Compression. Australasian Journal of Paramedicine, 5(3). Retrieved from http://ro.ecu.edu.au/jephc/vol5/iss3/2
10.4 Use of Oxygen in Emergencies
The changes to use of oxygen in emergencies have changed significantly after the research done by the UK Anaesthetics Society several years ago. Australia is now playing a bit of catch up regarding the use of oxygen. Unfortunately, there are some disparities and anomalies in the guidelines between the recommendations for ALS vs BLS. Whilst the ARC is aware of these anomalies, no changes have been made to address these issues. For example, the guideline states:
“When bag-valve-mask oxygen resuscitation is used by trained but occasional operators, a minimum of two trained rescuers are required to provide ventilation for a non-breathing victim.”
However many ALS operators would be considered “occasional” and there is no stipulation that they “are required” to use two operators. Surely the standard should be competence in one person ventilation (after all first aiders do not travel in groups for the most part) and on failure of this, then two-person (if available) delivery.
Conclusion
In reviewing the summary of changes in the 2016 ANZCOR Guidelines, it is apparent to ARAN that they have fallen short of their potential to promote improvement in casualty outcomes and better equip first aiders to provide effective, evidenced-based foundations to their care. The individual guidelines are inconsistent and contradictory in both terminology and the use of evidence on which is based recommendations and consensus view. It is apparent that many authors have controlled the review of individual sections, without a consistent approach to the purpose, implications and evidence required to inform consensus view over scientific literature and clinical findings. This misuse of evidence-based review leads to therapeutic nihilism (the belief that there is no objective basis for truth) in the absence of evidence from randomized trials.
Historically, highlighting issues such as these to the ARC and/or the submission of constructive, evidenced suggestions are met with silence. This is followed by complete dismissal (without explanation, discussion or the provision of counter evidence). This must suggest that to the observer, that the methodology of review and evidence used by the ARC is flawed, partisan and conceited. This unfortunately means that there is no current, effective means of influencing change in the ARC published guidelines in Australia regardless of one’s evidence and/or clinical standing (outside of its internal structure) and thus no peer review.
ARAN suggests that individuals (both clinical and non-clinical) closely review the new ANZCOR guidelines for themselves to determine their consistency and efficacy and then independently decide if the ARC Guidelines (opinions as published) are suitable and relevant for their individual situation.
Saving Lives in Schools and Sports - the facts about Automated External Defibrillators (AEDs) in NSW Schools
Australian Resuscitation Advisory Network
Introduction
At the Australian Resuscitation Advisory Network (ARAN), we are dedicated to improving the survival rates from cardiac arrest, a condition that strikes suddenly and can occur at any age. Over the years in NSW there has been reluctance by Government to the installation of AED(s) in schools, and NSW still remains the only state in Australia where schools are not actually encouraged to purchase an AED.
The official policy from the NSW Department of Education (DoE) relies on “formal advice” received from the Ministry of Health suggesting that AEDs are “not necessary” as Sudden Cardiac Arrest (SCA) among school age children and youths is, fortunately, infrequent. While statistically this is true, the fact that they occur at all (and result in death) for the sake of a simple piece of equipment - is tragic. Strangely, in our investigation into AEDs in NSW schools, the Ministry of Health denies giving such advice to the NSW Department of Education that AEDs in schools are “unnecessary”. Sadly, in Australia there is also no WHS legislation or codes of practice that require employers/workplaces to have AED(s) dependent on staff size, location or nature of their work, even if they have significant customer traffic (e.g. fast food chains) or identified high risk workplaces e.g. high voltage electrical work.
So why have a defibrillator in your school? Firstly, Sudden Cardiac Arrest (SCA) must be treated quickly (< 3 minutes) for a successful outcome and survival rates of 43—75% compared to the usual 5-6% in Australia. Regardless of the proximity of medical services to a school, this target time to defibrillation cannot be met without an AED located at the school. As of July 2016 only 25% of general practices in Australia have AEDs, hospitals do not loan out defibrillators in an emergency, and Ambulance response times in NSW average 9.3 minutes to the door (not the casualty).
Secondly, the presence of AEDs in schools, and AED programs, improve public awareness of what SCA is, what AEDs are, and the importance of immediate bystander action; particularly for the next generation. This occurs through the transfer of knowledge from students and staff to family and friends and by direct observation of parents and visitors who see and learn about AEDs when they visit the school. While most cardiac arrests in schools occur in adults—both staff and visitors - many, if not most schools serve as community meeting centres, and so sustain adult traffic during school and non-school hours.
Sadly, we know there are a significant number of young athletes with undetected, underlying heart disease that predisposes them to SCA, which is exacerbated at times of exertion. As no routine screening is done in Australia for these heart defects, the level of this risk is largely hidden until an event.
Unfortunately in NSW, AEDs are not a central focus in schools by government (as it is in other countries around the world) and NSW guidelines currently advise that they are “not a requirement for schools”. This advice is repeated no less than 4 times in bolded text in the Department of Education guidelines, and is extremely disappointing. However the document also demonstrates a lack of understanding of the importance of a community response to a very serious epidemic and the role and operation of modern defibrillators.
This document from ARAN provides easy-to-understand descriptions of how an AED works and the fundamental principles of an effective public access defibrillation (PAD) program in schools. Apart from the internal regulatory obligations imposed by the Department of Education, installing and maintaining an AED in a school is not the onerous task suggested in the school AED guidelines.
It is now time that we all work together to eliminate preventable deaths from SCA (33,000+ each year in Australia) that continue to occur all too often. Establishing emergency action plans in schools (and school sports programs) that include response planning, training in CPR, and deployment of AEDs and providing CPR and AED training to all students will greatly reduce the risk that we and our children will face from sudden cardiac arrest. This has been well proven in countries such as Ireland and Scotland where schools and community, local, state and federal Government work together on this issue.
Sudden Cardiac Arrest (SCA) Facts
No school principal, teacher, or sports coach wants to think about the prospect of the injury or death of a child who is under their supervision. Certainly no one working with young people would knowingly let them play on unsafe playground equipment, sit in a classroom that did not meet building codes, or participate in sports without the proper protective gear. The school first aid kit is expected to be stocked with bandages, cold packs, and other standard first aid supplies. Yet, every day in schools and on sports fields, many of our youth are left unprotected from sudden cardiac arrest – for which there is a simple-to-use device that is becoming a standard of care in public facilities, offices, health clubs, shopping centres, and even many schools.
Unfortunately, without widespread screening of young people for underlying heart conditions, there is always a risk of SCA amongst school age children. Studies have identified a 2.5 times relative risk for SCA attributable to sports activity in adolescent and young adult athletes versus an age-matched non-athletic population, related to underlying cardiac disorders.
In Australia, sudden cardiac arrest (SCA) strikes more than 33,000 people annually (more than 500 per week) and is the leading cause of death each year, killing more than stroke, breast cancer, lung cancer, and HIV/AIDS and motor vehicle accidents combined. While most SCA deaths occur in adults, SCA is also the leading cause of death in young athletes and can also strike children participating in normal school or sports activity. Even the most healthy-appearing competitive athletes and students may harbour unsuspected cardiovascular disease with the potential to cause sudden death. This unfortunately can happen without warning and in 25% of SCA cases the first sign is death.
SCA results from a disruption in the heart’s electrical system, which generally causes the heart to beat very rapidly and irregularly (ventricular fibrillation), a heart rhythm that does not pump blood to the brain, heart and other vital organs. Victims typically lose consciousness in a matter of seconds. Without immediate CPR compressions to help the heart continue to transport blood to and maintain the supply of oxygen to vital organs, and the shock of an AED to enable the heart’s natural rhythm, victims usually die. By the time an ambulance has arrived, it is often too late.
The good news is that the simplicity of AEDs makes rapid, public response possible. In Australia we are sadly lagging behind the rest of the world in preparing schools for these emergencies. Scotland has a nationally focused campaign to ensure all school children receive training in CPR (including AEDs) and in the US, more than 20 states and hundreds of school districts now require AEDs to be standard equipment.
HEART ATTACK
Many people (including the media) confused the term “heart attack” and “cardiac arrest”. A heart attack, or acute myocardial infarction (AMI), is caused by a circulation or plumbing problem of the heart, when one (or more) of the arteries delivering blood to the heart is severely restricted or blocked. Oxygen in the blood cannot reach the heart muscle, and the heart muscle becomes damaged.
• This damage to the heart muscle can lead to a malfunction of the heart’s electrical system, causing dangerously fast or slow heart rhythms that can cause a cardiac arrest, however most heart attack victims do not have cardiac arrests at the same time.
• Many SCAs occur in patients with coronary heart disease (70-80%). If the patient suffers a heart attack, there is a higher risk for SCA.
Symptoms of heart attack can include chest pain, radiating pain (left arm, between shoulder blades, jaw), difficulty breathing, dizziness, nausea and vomiting, and profuse sweating or may be completely symptom free (silent).
CARDIAC ARREST
Cardiac Arrest on the other hand is the cessation of effective heart function. In most cases of cardiac arrest, the heart initially does not stop but goes into a chaotic rhythm that does not result in blood being pumped to the brain and heart. The result is the same, in that death will shortly follow unless resuscitation (including the use of an AED) is started quickly. Cardiac arrest can also result from a lack of oxygen e.g. drowning, choking, asthma, where the heart slows to a stop. This is the most common form of cardiac arrest in younger children.
Why kids are at risk from sudden cardiac arrest?
There are several conditions and events that can be causes of sudden cardiac arrest. Some conditions are congenital, (present at birth). Among these conditions are Long QT Syndrome, Hypertrophic Cardiomyopathy (HCM), Brugada Syndrome, Wolff– Parkinson-White Syndrome, and Marfan Syndrome. It is estimated that 1 out of every 128 infants is born with congenital heart disease each year in Australia. Around 3000 babies are born each year with heart defects ranging from holes in the heart, leaky valves, or abnormalities in the heart chambers.
Some of these heart defects can prevent the heart from pumping a sufficient amount of blood to the lungs and other body organs, which can cause congestive heart failure. Other affected children may have rapid or irregular heartbeats and rhythms, and it may be difficult to breathe, especially during physical activity. The good news is that there are treatment options for these conditions if detected and diagnosed in time. However these children are at higher risk of SCA.
Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy, or HCM, is a genetic cardiac condition affecting one in 200 people. HCM causes the heart to become thick and the anatomy to be abnormal from the cellular level. HCM is the most common cardiac cause of sudden cardiac arrest in the young (under 35).
Long QT (and related syndromes)
Long QT is a disturbance of the heart’s electrical system, causing an abnormality of the heart’s rhythm. Because of this abnormality, those who are affected are susceptible to sudden fainting (syncope) and in some cases, death from SCA. Although most episodes occur during periods of physical exertion, they can occur during emotional stress or even sleep. Death from long QT syndrome is preventable through proper diagnosis and treatment.
Commotio Cordis
Commotio-cordis is a rare but potentially fatal phenomenon that can result in sudden cardiac arrest. It can occur when a blunt, (but often mild) blow to the area of the chest directly over the heart occurs during a precise moment of the heart’s cycle, leading to sudden cardiac arrest. It can occur both in contact sports and non-contact ball games.
Commotio-cordis is sometimes referred to as a “concussion of the heart” and is only treatable with CPR compressions and defibrillation to reverse ventricular fibrillation (a chaotic, life threatening heart rhythm) .
Other Causes
Electrolyte imbalances caused by eating disorders, rapid weight loss or dehydration e.g. distance running in a hot environment.
What is the difference between defibrillators (AEDs)?
Automatic vs Semi-Automatic
An Automated External Defibrillator (AED) comes in two basic configurations, Automatic and Semi-Automatic. Automatic defibrillators tell the rescuers it is about to shock, however if you don’t hear this message i.e. noisy environment or inattention, it shocks anyway. A Semi-Automatic defibrillator provides an additional safety step in that someone has to push the shock button when prompted i.e. visual check everyone is clear of the casualty. An inadvertent shock has the potential to cause a cardiac arrest in another person (other than the casualty).
Age range for defibrillators
AEDs are not designed to be used on a casualty under 12 months of age. In defibrillation terms an Adult is defined as a person > 8 years and a Child is defined as >1 year ≤ 8 years. Different defibrillation pads are usually needed for children < 8 years old.
Ongoing Costs
CPR Feedback - as good compressions are crucial in resuscitation, AEDs have a range of measures that can help maintain this. The simplest feedback measure is a metronome. Some defibrillators have patented compression feedback systems that use either an accelerometer or an algorithm that detects impedance changes.
Security
The guidelines from the DoE require schools to place an AED in a cabinet with a security alarm, however a standard cabinet with a security tag has proved to be an adequate measure with defibrillators placed in schools and other public places to discourage theft and/or vandalism.
Unfortunately the AED guidelines for schools restrict the purchase of AEDs from a limited list and provide no actual recommended specification or rationale for one AED feature over another. This list does not contain newer AEDs that are equally or more suitable for a school situation.
Other benefits of introducing a defibrillator to your school
Apart from purchasing a defibrillator for your school, there is great value in educating students about the role and use of an AED with CPR. The education of school children in CPR (including defibrillation) has been shown in many countries around the world to not only to improve outcomes in the community today, but also to have improved the willingness and capability of the individuals as they move from school into the community. In other words, education about AEDs and CPR supports a generational change in cardiac arrest outcomes through an increased willingness and ability to respond. There are numerous examples of children using the resuscitation life skills learned at school to save friends and relatives.
In one study researchers used a mock simulation of cardiac arrest to familiarise sixth-grade students who had no previous training with the use of an AED. They compared time to defibrillation, pad placement, and compliance with AED prompts to stand clear of the patient during shock delivery between the sixth year students and paramedics.
The mean time to defibrillation was 90 seconds for the year six students and 67 seconds for the professionals. Both the year six students and professionals placed the pads correctly and stood clear of the patient during shock delivery. In another study, Lawson et al assessed year three students use of an AED after explaining only the mechanics of peeling off the backing from the pads. Those students successfully used the AED on a manikin but, after a 2-minute, one-on-one orientation, their performance was significantly faster in a second trial. These studies prove the ease of AED use by even the very young and, in the latter instance, minimally trained users. High school AED programmes demonstrate a high survival rate (71%) for students and adults who suffer SCA on school grounds. School-based AED programmes are therefore strongly encouraged in current research.
Here is a handy risk assessment tool for staff http://www.scarisk.org/
At the Australian Resuscitation Advisory Network (ARAN), we are dedicated to improving the survival rates from cardiac arrest, a condition that strikes suddenly and can occur at any age. Over the years in NSW there has been reluctance by Government to the installation of AED(s) in schools, and NSW still remains the only state in Australia where schools are not actually encouraged to purchase an AED.
The official policy from the NSW Department of Education (DoE) relies on “formal advice” received from the Ministry of Health suggesting that AEDs are “not necessary” as Sudden Cardiac Arrest (SCA) among school age children and youths is, fortunately, infrequent. While statistically this is true, the fact that they occur at all (and result in death) for the sake of a simple piece of equipment - is tragic. Strangely, in our investigation into AEDs in NSW schools, the Ministry of Health denies giving such advice to the NSW Department of Education that AEDs in schools are “unnecessary”. Sadly, in Australia there is also no WHS legislation or codes of practice that require employers/workplaces to have AED(s) dependent on staff size, location or nature of their work, even if they have significant customer traffic (e.g. fast food chains) or identified high risk workplaces e.g. high voltage electrical work.
So why have a defibrillator in your school? Firstly, Sudden Cardiac Arrest (SCA) must be treated quickly (< 3 minutes) for a successful outcome and survival rates of 43—75% compared to the usual 5-6% in Australia. Regardless of the proximity of medical services to a school, this target time to defibrillation cannot be met without an AED located at the school. As of July 2016 only 25% of general practices in Australia have AEDs, hospitals do not loan out defibrillators in an emergency, and Ambulance response times in NSW average 9.3 minutes to the door (not the casualty).
Secondly, the presence of AEDs in schools, and AED programs, improve public awareness of what SCA is, what AEDs are, and the importance of immediate bystander action; particularly for the next generation. This occurs through the transfer of knowledge from students and staff to family and friends and by direct observation of parents and visitors who see and learn about AEDs when they visit the school. While most cardiac arrests in schools occur in adults—both staff and visitors - many, if not most schools serve as community meeting centres, and so sustain adult traffic during school and non-school hours.
Sadly, we know there are a significant number of young athletes with undetected, underlying heart disease that predisposes them to SCA, which is exacerbated at times of exertion. As no routine screening is done in Australia for these heart defects, the level of this risk is largely hidden until an event.
Unfortunately in NSW, AEDs are not a central focus in schools by government (as it is in other countries around the world) and NSW guidelines currently advise that they are “not a requirement for schools”. This advice is repeated no less than 4 times in bolded text in the Department of Education guidelines, and is extremely disappointing. However the document also demonstrates a lack of understanding of the importance of a community response to a very serious epidemic and the role and operation of modern defibrillators.
This document from ARAN provides easy-to-understand descriptions of how an AED works and the fundamental principles of an effective public access defibrillation (PAD) program in schools. Apart from the internal regulatory obligations imposed by the Department of Education, installing and maintaining an AED in a school is not the onerous task suggested in the school AED guidelines.
It is now time that we all work together to eliminate preventable deaths from SCA (33,000+ each year in Australia) that continue to occur all too often. Establishing emergency action plans in schools (and school sports programs) that include response planning, training in CPR, and deployment of AEDs and providing CPR and AED training to all students will greatly reduce the risk that we and our children will face from sudden cardiac arrest. This has been well proven in countries such as Ireland and Scotland where schools and community, local, state and federal Government work together on this issue.
Sudden Cardiac Arrest (SCA) Facts
No school principal, teacher, or sports coach wants to think about the prospect of the injury or death of a child who is under their supervision. Certainly no one working with young people would knowingly let them play on unsafe playground equipment, sit in a classroom that did not meet building codes, or participate in sports without the proper protective gear. The school first aid kit is expected to be stocked with bandages, cold packs, and other standard first aid supplies. Yet, every day in schools and on sports fields, many of our youth are left unprotected from sudden cardiac arrest – for which there is a simple-to-use device that is becoming a standard of care in public facilities, offices, health clubs, shopping centres, and even many schools.
Unfortunately, without widespread screening of young people for underlying heart conditions, there is always a risk of SCA amongst school age children. Studies have identified a 2.5 times relative risk for SCA attributable to sports activity in adolescent and young adult athletes versus an age-matched non-athletic population, related to underlying cardiac disorders.
In Australia, sudden cardiac arrest (SCA) strikes more than 33,000 people annually (more than 500 per week) and is the leading cause of death each year, killing more than stroke, breast cancer, lung cancer, and HIV/AIDS and motor vehicle accidents combined. While most SCA deaths occur in adults, SCA is also the leading cause of death in young athletes and can also strike children participating in normal school or sports activity. Even the most healthy-appearing competitive athletes and students may harbour unsuspected cardiovascular disease with the potential to cause sudden death. This unfortunately can happen without warning and in 25% of SCA cases the first sign is death.
SCA results from a disruption in the heart’s electrical system, which generally causes the heart to beat very rapidly and irregularly (ventricular fibrillation), a heart rhythm that does not pump blood to the brain, heart and other vital organs. Victims typically lose consciousness in a matter of seconds. Without immediate CPR compressions to help the heart continue to transport blood to and maintain the supply of oxygen to vital organs, and the shock of an AED to enable the heart’s natural rhythm, victims usually die. By the time an ambulance has arrived, it is often too late.
The good news is that the simplicity of AEDs makes rapid, public response possible. In Australia we are sadly lagging behind the rest of the world in preparing schools for these emergencies. Scotland has a nationally focused campaign to ensure all school children receive training in CPR (including AEDs) and in the US, more than 20 states and hundreds of school districts now require AEDs to be standard equipment.
HEART ATTACK
Many people (including the media) confused the term “heart attack” and “cardiac arrest”. A heart attack, or acute myocardial infarction (AMI), is caused by a circulation or plumbing problem of the heart, when one (or more) of the arteries delivering blood to the heart is severely restricted or blocked. Oxygen in the blood cannot reach the heart muscle, and the heart muscle becomes damaged.
• This damage to the heart muscle can lead to a malfunction of the heart’s electrical system, causing dangerously fast or slow heart rhythms that can cause a cardiac arrest, however most heart attack victims do not have cardiac arrests at the same time.
• Many SCAs occur in patients with coronary heart disease (70-80%). If the patient suffers a heart attack, there is a higher risk for SCA.
Symptoms of heart attack can include chest pain, radiating pain (left arm, between shoulder blades, jaw), difficulty breathing, dizziness, nausea and vomiting, and profuse sweating or may be completely symptom free (silent).
CARDIAC ARREST
Cardiac Arrest on the other hand is the cessation of effective heart function. In most cases of cardiac arrest, the heart initially does not stop but goes into a chaotic rhythm that does not result in blood being pumped to the brain and heart. The result is the same, in that death will shortly follow unless resuscitation (including the use of an AED) is started quickly. Cardiac arrest can also result from a lack of oxygen e.g. drowning, choking, asthma, where the heart slows to a stop. This is the most common form of cardiac arrest in younger children.
Why kids are at risk from sudden cardiac arrest?
There are several conditions and events that can be causes of sudden cardiac arrest. Some conditions are congenital, (present at birth). Among these conditions are Long QT Syndrome, Hypertrophic Cardiomyopathy (HCM), Brugada Syndrome, Wolff– Parkinson-White Syndrome, and Marfan Syndrome. It is estimated that 1 out of every 128 infants is born with congenital heart disease each year in Australia. Around 3000 babies are born each year with heart defects ranging from holes in the heart, leaky valves, or abnormalities in the heart chambers.
Some of these heart defects can prevent the heart from pumping a sufficient amount of blood to the lungs and other body organs, which can cause congestive heart failure. Other affected children may have rapid or irregular heartbeats and rhythms, and it may be difficult to breathe, especially during physical activity. The good news is that there are treatment options for these conditions if detected and diagnosed in time. However these children are at higher risk of SCA.
Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy, or HCM, is a genetic cardiac condition affecting one in 200 people. HCM causes the heart to become thick and the anatomy to be abnormal from the cellular level. HCM is the most common cardiac cause of sudden cardiac arrest in the young (under 35).
Long QT (and related syndromes)
Long QT is a disturbance of the heart’s electrical system, causing an abnormality of the heart’s rhythm. Because of this abnormality, those who are affected are susceptible to sudden fainting (syncope) and in some cases, death from SCA. Although most episodes occur during periods of physical exertion, they can occur during emotional stress or even sleep. Death from long QT syndrome is preventable through proper diagnosis and treatment.
Commotio Cordis
Commotio-cordis is a rare but potentially fatal phenomenon that can result in sudden cardiac arrest. It can occur when a blunt, (but often mild) blow to the area of the chest directly over the heart occurs during a precise moment of the heart’s cycle, leading to sudden cardiac arrest. It can occur both in contact sports and non-contact ball games.
Commotio-cordis is sometimes referred to as a “concussion of the heart” and is only treatable with CPR compressions and defibrillation to reverse ventricular fibrillation (a chaotic, life threatening heart rhythm) .
Other Causes
Electrolyte imbalances caused by eating disorders, rapid weight loss or dehydration e.g. distance running in a hot environment.
What is the difference between defibrillators (AEDs)?
Automatic vs Semi-Automatic
An Automated External Defibrillator (AED) comes in two basic configurations, Automatic and Semi-Automatic. Automatic defibrillators tell the rescuers it is about to shock, however if you don’t hear this message i.e. noisy environment or inattention, it shocks anyway. A Semi-Automatic defibrillator provides an additional safety step in that someone has to push the shock button when prompted i.e. visual check everyone is clear of the casualty. An inadvertent shock has the potential to cause a cardiac arrest in another person (other than the casualty).
Age range for defibrillators
AEDs are not designed to be used on a casualty under 12 months of age. In defibrillation terms an Adult is defined as a person > 8 years and a Child is defined as >1 year ≤ 8 years. Different defibrillation pads are usually needed for children < 8 years old.
Ongoing Costs
- Maintenance— Modern AEDs do not require ongoing maintenance. The machines are self-monitoring and reporting. The AED will indicate when it need attention and most will tell you the problem. A weekly check that there are no warning lights present and that the pads are in date is all that is required.
- Warranty - Most AEDs have an expected service life of up to 10 years so the warranty should meet or exceed this.
- Battery Life - battery life can range between models and manufactures from around 2 years up to 7 years.
- Cost of Consumables - specialised battery packs can cost from $90.00 to $280.00 . Replacement adult pads range from $90.00 to $150.00, while paediatric pads are more expensive with costs ranging from $92.00 to around $200.00. All pads have a maximum of a 4 year shelf life (usually up to 2 1/2 years).
CPR Feedback - as good compressions are crucial in resuscitation, AEDs have a range of measures that can help maintain this. The simplest feedback measure is a metronome. Some defibrillators have patented compression feedback systems that use either an accelerometer or an algorithm that detects impedance changes.
Security
The guidelines from the DoE require schools to place an AED in a cabinet with a security alarm, however a standard cabinet with a security tag has proved to be an adequate measure with defibrillators placed in schools and other public places to discourage theft and/or vandalism.
Unfortunately the AED guidelines for schools restrict the purchase of AEDs from a limited list and provide no actual recommended specification or rationale for one AED feature over another. This list does not contain newer AEDs that are equally or more suitable for a school situation.
Other benefits of introducing a defibrillator to your school
Apart from purchasing a defibrillator for your school, there is great value in educating students about the role and use of an AED with CPR. The education of school children in CPR (including defibrillation) has been shown in many countries around the world to not only to improve outcomes in the community today, but also to have improved the willingness and capability of the individuals as they move from school into the community. In other words, education about AEDs and CPR supports a generational change in cardiac arrest outcomes through an increased willingness and ability to respond. There are numerous examples of children using the resuscitation life skills learned at school to save friends and relatives.
In one study researchers used a mock simulation of cardiac arrest to familiarise sixth-grade students who had no previous training with the use of an AED. They compared time to defibrillation, pad placement, and compliance with AED prompts to stand clear of the patient during shock delivery between the sixth year students and paramedics.
The mean time to defibrillation was 90 seconds for the year six students and 67 seconds for the professionals. Both the year six students and professionals placed the pads correctly and stood clear of the patient during shock delivery. In another study, Lawson et al assessed year three students use of an AED after explaining only the mechanics of peeling off the backing from the pads. Those students successfully used the AED on a manikin but, after a 2-minute, one-on-one orientation, their performance was significantly faster in a second trial. These studies prove the ease of AED use by even the very young and, in the latter instance, minimally trained users. High school AED programmes demonstrate a high survival rate (71%) for students and adults who suffer SCA on school grounds. School-based AED programmes are therefore strongly encouraged in current research.
Here is a handy risk assessment tool for staff http://www.scarisk.org/
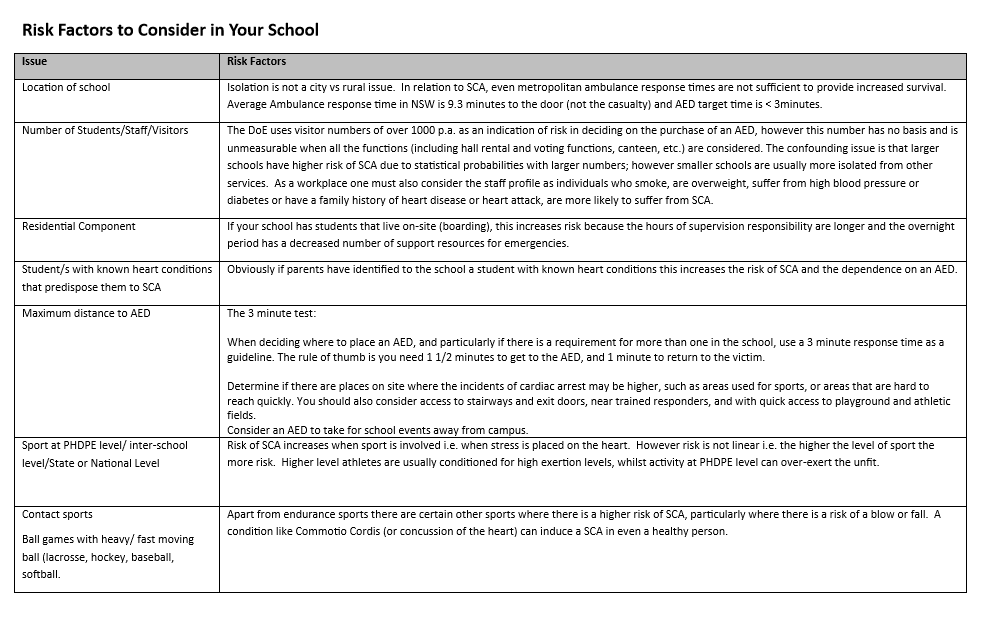
Funding a Defibrillator
An AED and the necessary accessories, doesn’t come without a cost. At present, the cost of an AED is borne by the school as is any consumables that need to be replaced. The purchase of a defibrillator is an important issue for parents at the school and so the P&C is a logical place to start to focus fund raising efforts. The purchase and installation of an AED in the local school has a high community interest. Promotion of such an initiative is likely to bring positive attention and support from the community and media.
There are also some organisations that have programs to support the purchase of defibrillators in the community. In other countries, like the UK, Government and private grants are available for the purchase of defibrillators for schools. There are also corporations that are willing to sponsor an AED for schools.
The Department of Education in the UK has also produced more detailed and helpful guidelines to also assist schools with purchasing and maintaining AEDs.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/519994/AED_guide_for_schools.pdf
Final Tips
The 3 keys to operating an AED are:
An AED should be in a location where it can be accessed by the public during out-of-hours functions. Security for the AED does not need to be over-the-top and breakable security tags have proven to be effective measures in public places across Australia. Alternatively a “break box for key” arrangement could be employed, however this increases response time.
Conclusion
The reality of cardiac arrest is that is usually has a very poor outcome if we rely on Ambulance response and CPR. The best chance a casualty has in SCA is early defibrillation (using an AED) combined with fast deep compressions. Modern AEDs do not require any special training to operate and all basic CPR training in Australia includes the operation of a defibrillator (AED). Ambulance operators are also trained to guide you through the operation of the AED in an emergency.
Despite the general lack of enthusiasm by Government regarding schools in NSW installing defibrillators, they remain the most effective measure for a positive outcome in the tragic event of SCA. Hopefully, after reading this document you have a more thorough and balanced understanding of AEDs, and will be able to appreciate that an AED is not just an “unnecessary” complication to your school, but both a valuable and necessary part of a modern education system, and in the best interests of students, staff and the community.
An AED and the necessary accessories, doesn’t come without a cost. At present, the cost of an AED is borne by the school as is any consumables that need to be replaced. The purchase of a defibrillator is an important issue for parents at the school and so the P&C is a logical place to start to focus fund raising efforts. The purchase and installation of an AED in the local school has a high community interest. Promotion of such an initiative is likely to bring positive attention and support from the community and media.
There are also some organisations that have programs to support the purchase of defibrillators in the community. In other countries, like the UK, Government and private grants are available for the purchase of defibrillators for schools. There are also corporations that are willing to sponsor an AED for schools.
The Department of Education in the UK has also produced more detailed and helpful guidelines to also assist schools with purchasing and maintaining AEDs.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/519994/AED_guide_for_schools.pdf
Final Tips
The 3 keys to operating an AED are:
- An AED is most effective when used in combination with fast deep compression (although compressions should be ceased whilst the AED is diagnosing and delivering a shock – the machine will remind you of this)
- All AEDs should have a skin preparation kit with the machine. This should include:
- A pair of trauma scissors to remove the clothing on the chest quickly
- A safety razor to remove any excess hair from the pads placement area
- A disposable towel to wipe down the skin to remove moisture
- Ensure no one is touching the casualty when a shock is delivered. The AED will tell you to “STAND CLEAR” when it is charging up ready to shock.
An AED should be in a location where it can be accessed by the public during out-of-hours functions. Security for the AED does not need to be over-the-top and breakable security tags have proven to be effective measures in public places across Australia. Alternatively a “break box for key” arrangement could be employed, however this increases response time.
Conclusion
The reality of cardiac arrest is that is usually has a very poor outcome if we rely on Ambulance response and CPR. The best chance a casualty has in SCA is early defibrillation (using an AED) combined with fast deep compressions. Modern AEDs do not require any special training to operate and all basic CPR training in Australia includes the operation of a defibrillator (AED). Ambulance operators are also trained to guide you through the operation of the AED in an emergency.
Despite the general lack of enthusiasm by Government regarding schools in NSW installing defibrillators, they remain the most effective measure for a positive outcome in the tragic event of SCA. Hopefully, after reading this document you have a more thorough and balanced understanding of AEDs, and will be able to appreciate that an AED is not just an “unnecessary” complication to your school, but both a valuable and necessary part of a modern education system, and in the best interests of students, staff and the community.
The five specific “diseases” that are infecting science
John Antonakis (psychologist and researcher)
John Antonakis (psychologist and researcher)
- Significosis is the incessant focus on producing statistically significant results, a well-known problem but one that still plagues us. Because the players in the publication game only consider statistically significant results as interesting and worthwhile to publish, the distribution of effect sizes is highly skewed. The potentially wrong estimates feed into meta-analyses and then inform policy. A result could be significant for many reasons, including chance or investigator bias, and not because the effect is true.
- Neophilia is about an excessive appreciation for novelty and for snazzy results. There is nothing per se wrong with novel findings, but these are not the only findings that are useful; and, of course, sometimes novel findings turn out to be false. Replications of a previous effect, for instance, may not seem very interesting at the outset; but they are critical to helping understand if an effect is present or not. Many journals simply do not consider publishing replications, which I find disturbing. In my field, I am rather certain that many published findings and theories are flawed; however, they will never be challenged if replications—and null results studies too—are never published.
- Theorrhea refers to a mania for new theory is something that afflicts many branches of social science. That is, there is usually a requirement in top journals to make a new contribution to theory, and that research should be theory driven and not exploratory. How is it possible that we can have so many contributions to theory? Imagine just in the field of management research, having say 5 elite journals, each publishing 80 papers a year. How is it possible to produce several hundred new contributions to theory every year, as compared say to physics, which has very strong theoretical foundations, but operates more slowly in terms of theory development and also appreciates basic research?
- Arigorium concerns a deficiency of rigor in theoretical and empirical work. The theories in my field, and in most of the social sciences too, save economics and some branches of political science and sociology, are very imprecise. They need to be formalized and not produced on the “cheap” and in large quantities. They must make more precise, realistic, and testable predications. As regards empirical work, there is a real problem of failing to clearly identify causal empirical relations. A lot of the work that is done in many social sciences disciplines is observational and cross sectional and there is a dearth of well-done randomized controlled experiments, either in the field or the laboratory, or work that uses robust quasi-experimental procedures.
- Disjunctivitis is a disease that is about a collective proclivity to produce large quantities of redundant, trivial, and incoherent works. This happens because of several reasons, but primarily because quantity of publications is usually rewarded. In addition, researchers have to stake a name for themselves; given that novelty, significance results, and new theory are favored too means that a lot of research is produced that is disjointed from an established body of knowledge. Instead of advancing in a paradigmatic fashion, researchers each take little steps in different directions. Worse, they go backwards or just run on the spot and do not achieve much. The point is that the research that is done is fragmented and is not helping science advance in a cohesive fashion. Findings must be synthesized and bridges must be built to other disciplines (e.g., evolutionary biology) so that we can better understand how the world works.
The Dichotomy in the Australian Resuscitation Council
With a catchphrase of “Any attempt at resuscitation is better than no attempt” but aims and objectives that seek to control standardisation in Australia and New Zealand; how committed is the Australian Resuscitation Council to better outcomes as opposed to control over resuscitation practice and teaching?
This dichotomy has perhaps hamstrung improvements in OHCA outcomes in Australia for years and seen us languishing behind the rest of the world. The fundamental belief that must be assumed, (in order to enable these opposing concepts to co-exist), is that the ARC guidelines and consensus opinion is unquestionably “right”, at all times. It is quite evident that the stated aim in regard to “uniformity and standardisation” is the overriding philosophy, the driver of actions and that any notion of “any resuscitation attempt be better than none” only (and will forever only) refer to attempts that are made in conforming to ARC sanctioned, standardised recommendations.
“Aim: Foster and co-ordinate the practice and teaching of resuscitation promote uniformity and standardisation of resuscitation; act as a voluntary co-ordinating body” – ANZCOR Aims and Objectives.
In order to claim this infallibility, the ARC uses its objectives to give the appearance that its consensus opinion is the only correct interpretation of current research and evidence, restricts any input into resuscitation practice to the members of its own organisation, prosecutes (with apparent impunity) any view or solution that has not originated from its own deliberations and then the ARC fails to exercise due diligence to ensure recommendations are show the expected efficacy when applied i.e. there is a lack of accountability despite a demand for conformity. This methodology may be acceptable in a non-scientific environment but merely acts as a handbrake on genuine improvements in survival. That aside, if this methodology was effective at achieving best practice and results, this would be in evidence in outcome data, however this is not the case in Australia where the things measured don’t show a significant improvement over other approaches and those things not measured we will never know if recommendations result in help or harm.
How are the objectives used and misused to promote conformity and standardisation over ultimate improvement. If we number these 1 through 10 we can see this more clearly.
There are no less than nine areas where the ARC can improve its structure and practices to realise the spirit of its aims and objectives rather than what it has become:
As consumers of the guidelines and consensus opinions of the ARC (as Government and industry are also); we should demand that changes are made to the organisation if it is to continue to claim to be the “authority” on resuscitation practice in Australia and New Zealand. This includes meaningful and significant changes to governance structures, processes and focus.
Resuscitation outcomes are the concern of many individuals and organisations across the community, health and government. No one group has a monopoly on evidence, ideas and best practice. Particularly in Australia, where government (State and Federal) have no interest in improving OHCA survival rates outside their statutory obligations in the provision of ambulance and hospital services; it is incumbent on voluntary, not-for-profit organisations and individuals to all work toward the common goal of improving survival rates.
Simon Gould
Chairman – Australian Resuscitation Advisory Network
This dichotomy has perhaps hamstrung improvements in OHCA outcomes in Australia for years and seen us languishing behind the rest of the world. The fundamental belief that must be assumed, (in order to enable these opposing concepts to co-exist), is that the ARC guidelines and consensus opinion is unquestionably “right”, at all times. It is quite evident that the stated aim in regard to “uniformity and standardisation” is the overriding philosophy, the driver of actions and that any notion of “any resuscitation attempt be better than none” only (and will forever only) refer to attempts that are made in conforming to ARC sanctioned, standardised recommendations.
“Aim: Foster and co-ordinate the practice and teaching of resuscitation promote uniformity and standardisation of resuscitation; act as a voluntary co-ordinating body” – ANZCOR Aims and Objectives.
In order to claim this infallibility, the ARC uses its objectives to give the appearance that its consensus opinion is the only correct interpretation of current research and evidence, restricts any input into resuscitation practice to the members of its own organisation, prosecutes (with apparent impunity) any view or solution that has not originated from its own deliberations and then the ARC fails to exercise due diligence to ensure recommendations are show the expected efficacy when applied i.e. there is a lack of accountability despite a demand for conformity. This methodology may be acceptable in a non-scientific environment but merely acts as a handbrake on genuine improvements in survival. That aside, if this methodology was effective at achieving best practice and results, this would be in evidence in outcome data, however this is not the case in Australia where the things measured don’t show a significant improvement over other approaches and those things not measured we will never know if recommendations result in help or harm.
How are the objectives used and misused to promote conformity and standardisation over ultimate improvement. If we number these 1 through 10 we can see this more clearly.
- Provide a forum for discussion of all aspects of resuscitation – the forum for discussion is only internal i.e. within the organisation or affiliates. As the organisation is overseen by clinicians, there are many subjects that are not open to discussion or meaningful input from even the lower levels of their own organisation. No discussion is encouraged with anyone outside the organisation (not affiliated) and the strategy for dealing with any outside input is not to acknowledge or respond to any communication. There is no meaningful consultation outside its own network.
- Foster interest in, and promulgate information regarding resuscitation- whilst the ARC, in a limited and controlled way, spreads information regarding resuscitation., it is very careful to make the distinction between promotion for the overall good of the community and promotion of its own consensus view on resuscitation; the latter being the given priority. This means that internationally proven strategies and recommendations will never be promoted by the ARC if they somehow conflict with its own consensus view.
- Gather and collate scientific information regarding resuscitation techniques; to recommend a modification of those techniques where appropriate on the basis of such information – interestingly, “information” as mentioned here would never be the basis for change by the ARC. Rather, it maintains that change will only happen if it is based on “evidence” rather than “information”. The exception to this rule is when a technique without evidence is generated from within the ARC, and then the rules of evidence are suspended to allow information to have the same rigour.
- Promote simplicity and uniformity in techniques and terminology regarding resuscitation – whilst this may be the intent, the imperative for uniformity will always be the priority over simplicity in ARC commendations. The other aspect to this objective is the reality that simplicity does not automatically mean efficacy.
- Provide an advisory and resource service regarding techniques, equipment, teaching methods and teaching aids- this objective is part of the formulation and publication of its recommendations. One would therefore doubt that the ARC has no capacity (due to the imperative of maintaining its “proven” position ) to provide advice outside its internally accepted position, even if the particular circumstance is not adequately addressed by existing recommendations or where there is evidence that the technique or teaching method is flawed and ineffective.
- Foster research into methods of teaching and practice of resuscitation- this objective is extremely limited in its scope. As the organisation self-determines which “research” or “evidence” or” information” is valid to affect change, the research encouraged is that which supports the current position of the organisation. Anything with a contrary finding is deemed of insufficient rigour to influence change.
- Pursue the development of standards for training- there is no doubt that one of the prime ways the ARC maintains its primary imperative of conformity with its position is in the stranglehold it has on standards of training in Australia. Without any government authority, the ARC only has such “authority” that is given to it by other government and industry organisations in assenting to its recommendations as a de-facto standard for training. This position has remained unchallenged for many years, under the assumption that ARC recommendations represent the benchmark. Not surprisingly, any challenge to the status of the recommendations as not representing “best practice” in training are met with a vehement defence, not directly, but by using political and sector influence to stifle a threat to conformity, even if alternatives provide better outcomes.
- Establish regular communications with other bodies with similar objectives, both in Australia and overseas – this objective is simply disingenuous. Having “similar objectives” is not the criteria used by the ARC to determine communication. Rather, the ARC is in communication with bodies that support its “authority” and veracity of its recommendations. The ARC will not engage in any communication or initiatives with any organisation or individual that is not fully supportive of its unquestioned authority, regardless of community benefit.
- Consider and advise on the means of preventing circumstances in which resuscitation may become necessary- this objective is shared by many organisation involved in resuscitation, both in Australia and internationally. The dichotomy in the ARC is further exemplified by its approach to this objective. Identifying the “means of preventing circumstances….”, is an important function and many bodies have implemented strategies that have produced improvements in outcomes, however the difference with the ARC is that the only remedies it will recommend for implementation are those that it has dictated as in harmony with its own consensus and therefore advice is limited to advice that consolidates its position and control i.e. conformity.
- Do all such acts and things as are incidental, or subsidiary to all or any of the above objectives- to defend their position (of de-facto authority rather than the provision of evidenced recommendations), the ARC will apparently use any means, including the use of libel. To meet these objectives the ARC states that it:
- Develops and publishes Guidelines- this is a fundamental role of any resuscitation body. In reality, guidelines cannot be current at all times (unless they are constantly reviewed). Whilst a single set of guidelines may simplify practice, the assumption that must be made is that this solitary is both applicable in all circumstances and is an accurate distillation of international consensus and more importantly, evidence. With no review of outcomes from recommendations and no accountability for sub-standard recommendations; one guideline is in fact as good as any other guideline. However, one only has to produce an alternative guideline to experience the veracity in which the ARC defends its own guidelines as the only interpretation of evidence and international consensus with only its own consensus as the proof. While the defence may be the reliance on ILCOR recommendations, the ARC has demonstrated on more than one occasion that it is willing to go against international recommendations if its own local consensus has another opinion.
- Reviews and updates guidelines by consultation with member bodies and other experts- as already outlined any consultation is extremely selective and rooted in nepotism. Consultation is only effective if the input from those consulted has a role in forming or reforming the subject and its content or direction. If we look back at “consultation” phases of guidelines (which do not include those outside ARC affiliated bodies) contributors would be hard pressed to find a single submission that has resulted in any (even minute) change to a draft or proposal.
- Reviews world literature and research in resuscitation- if the reliance is on local consensus in the interpretation of international research i.e. what is commonly referred to as Level 4 evidence or expert opinion; then the validity of any recommendation is purely subjective and rigour only comes from ones opinion of the relevant “expert” making the recommendation. Reviews of world literature (especially where there are conflicting or weak results) can result in differing views on remedies, solutions and recommendations. Each of these may be equally as valid, however the stance of the ARC is that only their interpretation is valid (even if contrary to international consensus on evidence) and that no-one can question this or suggest another pathway. This approach is unscientific and experience has shown research discussion used by the ARC in place of research outcomes and recommendations as justification for a recommendation view. As the ultimate opinion that influences change within the ARC is solely that of medical practitioners, it is also not surprising that (particularly in BLS practice) recommendations reflect a hospital-centric view and world “evidence” is used in a selective and perverse manner as a justification to de-value pre-hospital measures.
- Act as a resource for anyone wanting authoritative material on resuscitation- as already established, the underlying requirement for acting as an “authority” is that the one seeking guidance must view the material and recommendations produced as being accurate and evidence-based practice. “Authoritative material” also assumes that anything not produced by the ARC lacks this “authority” and is therefore inferior and not evidence-based. This position is both arrogant and an example of poor governance. Opinion where there is no strong and definitive evidence cannot be elevated to a status of authoritative, regardless of the self-belief of the individuals formulating this opinion.
There are no less than nine areas where the ARC can improve its structure and practices to realise the spirit of its aims and objectives rather than what it has become:
- Improved governance – a weakness and misdirected governance is at the root of the issues identified. Elements of governance that need to be addressed include:
- Use of evidence and opinion – this has become clouded and political.
- This includes redefining LOE to reflect an accurate representation of consensus vs. evidence.
- Codes of conduct around the misuse of research or weighting of personal opinion over real evidence.
- Communication dysfunction – interaction with other organisations and individuals is dysfunctional at best and toxic at worst. This situation does not contribute to the ARC’s reputation in a positive way.
- Addressing questionable practices in response to criticism – there is an inability to constructively respond to valid criticism other than silence or personal attacks. Strong governance would insist on a more constructive methodology.
- Effective feedback and complaints management processes and accountabilities – at present there are no recognised processes in place to deal with feedback and there is no accountability for actions or no actions.
- Transparency
- A move from a “control of standardisation” approach to a “community benefit” approach
- Use of evidence and opinion – this has become clouded and political.
- Broader and meaningful consultation – internal and individual opinion (especially where evidence is weak, non-existent or conjectured) does not necessarily result in the best outcome.
- Review of the consequences of recommendations – recommendations, especially when based on local consensus need to be more closely monitored for efficacy in practice.
- User compatibility testing of recommendations (prior to release) – like most systems, any guidelines need to be usable by the end-user (not just the authors).
- Increased accountability for recommendations – without accountability for errors, recommendations can be merely experimental with no monitoring; this is poor scientific methodology.
- Government representation/ oversight – one cannot help but feel that a voluntary body that uses a group of individuals to make guidelines that areas of government and industry are forced to follow, show have some sort of government representation and/or oversight. This could and should also lead to funding opportunities. The notion of independence from political influence is the argument against this move; it could be easily argued that there exists more political influence from individuals and affiliates with agenda within the ARC itself.
- Innovation focus – what has been lost in the ARC in a quest for conformity is the ability to embrace innovation in a meaningful way.
- Efficacy rather than consensus – in the real world consensus is not a replacement for evidence or efficacy. This is regardless of whom the consensus is developed by. The notion of unquestionable consensus is a dangerous and unscientific approach, especially to resuscitation practice. Having witnessed first-hand at least the ARC process at state level; there is perhaps more rigour and less personal bias at an industrial union meeting. One can only assume that this behaviour is replicated at all levels of the organisation and would explain the behaviours of the current state and national bodies. Presently, some elements of ARC practice are contrary to international consensus and so local consensus has supplanted all other evidence without any proof of efficacy.
- Constant review methodology (in line with ILCOR) rather than structured and inflexible cycles - As ILCOR has realised that the irregular review of guidelines does not address the rapidly changing area of guideline development in resuscitation, the ARC needs also needs to move to a better methodology and process for review.
As consumers of the guidelines and consensus opinions of the ARC (as Government and industry are also); we should demand that changes are made to the organisation if it is to continue to claim to be the “authority” on resuscitation practice in Australia and New Zealand. This includes meaningful and significant changes to governance structures, processes and focus.
Resuscitation outcomes are the concern of many individuals and organisations across the community, health and government. No one group has a monopoly on evidence, ideas and best practice. Particularly in Australia, where government (State and Federal) have no interest in improving OHCA survival rates outside their statutory obligations in the provision of ambulance and hospital services; it is incumbent on voluntary, not-for-profit organisations and individuals to all work toward the common goal of improving survival rates.
Simon Gould
Chairman – Australian Resuscitation Advisory Network
Critical Review of the new ANZCOR Guideline 9.2.9 – First aid Management of a Diabetic Emergency released Nov. 2017
ARAN recently received notification that the new Diabetic Emergency Management guideline had been released by the ARC. On a first read it would appear that (like the recent AED position statement) someone from outside of the ARC perhaps should have been involved in proof reading this document before its release and those consuming the information consulted as to whether the document is logical and consistent from a first aid practice perspective i.e. that the guideline in in harmony with other guidelines in regard to advice and warnings.
As it is apparent these steps were not taken, let us list the obvious issues with this guideline. We do this in the full knowledge that any errors highlighted will not be corrected by the authors or certifiers as this would be considered an admission of error over an valid improvement in patient outcome.
As there is not a feedback process in place as to the actual efficacy of these measures once applied and no review mechanism to ensure safety and accuracy, this guideline will remain unchanged for the foreseeable future, regardless of any negative impact or concerns. To wit, no liability or responsibility will be taken by the ARC for any negative outcomes or errors as a result of their consensus opinions. ARAN will continue to provide critical review and alternative guidance for those interested in excellence in resuscitation.
Simon Gould - Chairman of the Australian Resuscitation Advisory Network (ARAN)
ARAN recently received notification that the new Diabetic Emergency Management guideline had been released by the ARC. On a first read it would appear that (like the recent AED position statement) someone from outside of the ARC perhaps should have been involved in proof reading this document before its release and those consuming the information consulted as to whether the document is logical and consistent from a first aid practice perspective i.e. that the guideline in in harmony with other guidelines in regard to advice and warnings.
As it is apparent these steps were not taken, let us list the obvious issues with this guideline. We do this in the full knowledge that any errors highlighted will not be corrected by the authors or certifiers as this would be considered an admission of error over an valid improvement in patient outcome.
- From a simple formatting view, paragraph 4.1 on the use of a glucometer needs to appear at the start of the document as:
- There is no mention in BSL as part of the diagnosis of hypoglycemia or hyperglycemia (< 3mmol/L or >15mmol/L in the body of the text, including in paragraphs 2.2 and 3.2 (Recognition of Low or High Blood Sugar). Whilst these levels reflect current evidence and practice they need to be mentioned in recognition rather than in a paragraph referring to "what if you don't know"?
- The underlying message that should be prominent in this guideline for first-aiders rather than health professionals is the age old truth, that "perfusion determines treatment" BSL is somewhat subjective and some casualties can have higher BSL's but be semi-conscious and conversely a casualty can have a BSL in the treatable hypoglycemic range but have not cognitive or physiological symptoms.
- The indication for the use of Glucagon is not by definition "a person with severe hypoglycemia" but rather by the text's own admission, and at a minimum, a casualty who has a low BSL (presumably <3mmol/L although not stated) and cannot swallow properly. A status of "severe hypoglycemia is not described in the document as a definable condition over "hypoglycemia" that needs to be treated.
- Paragraph 2.3 Management of Low Blood Sugar is of concern if this regime is expected to be carried out by non-clinically trained first-aiders. The preference stated to insert large hard objects (including Mentos, 5-10 no less) into potentially a child's mouth that someone assumes has an adequate gag reflect (and without anyway of of assessing) is at best foolish. At least this action should be prefaced with a test procedure (like a small sip of liquid first) and an appropriate warning. The preference for tablets and other hard choke inducing objects over glucose gel for first-aiders (that is absorbed through the mucus membranes rather than relying on swallowing); is of some concern. While it is noted that all measures involving hard tablets or lollies are acknowledged as having low or very low evidence (presumable on medication effectiveness only), there inclusion as the primary measures constitutes at least a casual reference to the Choking Guideline if not serious re-consideration.
- Paragraphs 3.1 and 3.2 assume hyperglycemia onset is usually a condition that first aiders will recognise. Most hyperglycemia is in diagnosed diabetic patients and is usually always associated with a concomitant illness, a fact not mentioned in the text.
As there is not a feedback process in place as to the actual efficacy of these measures once applied and no review mechanism to ensure safety and accuracy, this guideline will remain unchanged for the foreseeable future, regardless of any negative impact or concerns. To wit, no liability or responsibility will be taken by the ARC for any negative outcomes or errors as a result of their consensus opinions. ARAN will continue to provide critical review and alternative guidance for those interested in excellence in resuscitation.
Simon Gould - Chairman of the Australian Resuscitation Advisory Network (ARAN)
Silence not Science – How a Hypothesis becomes the only “truth”
The cautionary tale of the lack of debate and rigorous scientific, critical review in the Australian resuscitation community, compared to the perpetuation of the misguided Ancel Keys, Fat/Cholesterol = Heart Disease Hypothesis.
Whilst we may believe that pure scientific review is devoid of the contradictions and compromise of politics, the reality is somewhat different. Throughout history and to the present day many other factors influence what we believe to be true, acceptable and evidence-based, other than the pure scrutiny of scientific method. The Keys, fat and cholesterol hypothesis and their relationship to heart disease (except in a few individuals with genetic predispositions) has been the predominant thinking for decades in population medicine. It is central to government health messages, has built an enormous and lucrative low-fat industry, is instilled in the population from a young age and used to guide treatment by clinicians the world over. However, the evidence now indicates this hypothesis is and always was, wrong. Not that there is just new evidence so much that outranks the evidence used to support this hypothesis originally but that it has become apparent that the interpretation of the evidence was flawed, biased and based on the a desire by a few individuals to “own” the accepted wisdom and the status that necessarily brings.
The acceptance of the fat-cholesterol-heart disease hypothesis, if not based on sound, unquestionable, strong evidence, then how did it become the predominate view that crushed any alternate interpretation, evidence or questioning for decades? The strongest factors in the absence of good science in establishing the accepted wisdom were more related to who one managed to convince in key political positions, the veracity of efforts to discredit dissenting views, in creating a message that to the unscientific mind of the public would sound simple and logical enough to be accepted without question and lastly the phenomena whereby once out of the box, a theory gains momentum against all other challenges, regardless of its strength and rigour.
This timely example of the Keys hypotheses, should be a salient and lasting lesson to the scientific community as to the dangers in defending dogma rather than accepting that the re-examination of evidence or new findings can both lead to the discovery that the “accepted wisdom” is not in fact wisdom at all; or may be the result of other motives.
Resuscitation, particularly in Australia, is not immune to influences other than evidence in forming the accepted wisdom and dogma in practice. Some of this is apparent in other countries, but in Australia it is apparent that the organisation that the community looks to for guidance on resuscitation (The Australian Resuscitation Council - ARC), has developed a culture where dogma can survive without objective scrutiny and where politics and power are more important to some than the objective of saving lives.
There are several disturbing similarities between the success (only measured by acceptance rather than health outcomes) of the Keys Fat/Heart Disease Hypothesis and the ARC CPR/BLS Hypothesis evolution.
1. A fundamental and defended believe that the only ones worthy and presumably qualified of questioning the science are within the supporting organisation. Any request for further evidence is met with silence rather than science.
2. Prosecuting that the eminence of those supporting or promoting the view automatically means a position is true and above question.
3. Work to ensure any interpretation of evidence showing a differing position is dismissed as irrelevant and excluded from review.
4. Treat any individual showing dissent from the excepted wisdom with ridicule and is defamed.
5. Institute a policy whereby external enquiry in met with silence not science.
6. Establish yourself as “the authority”, the assumed source of “wisdom” and approval (with or without evidence) by regulatory means.
7. Restrict debate to those who accept the hypothesis or are sympathetic to it.
8. Modify process to ensure the protection of opinion over science.
The reader may not of course readily accept that the similarities are accurate or possible or that they have had any influence on the ultimate goal of survival from cardiac arrest in Australia. However, my personal experience and that of other organisations involved in saving lives, professional bodies, clinicians, training providers and even those in the ARC is that these similarities are not just possible but are very real and damaging in the ARC. Let us look more closely at the specifics of these experiences.
A fundamental and defended believe that the only ones worthy and presumably qualified of questioning the science are within the supporting organisation. Any request for further evidence is met with silence rather than science - the behaviour of the ARC clearly reinforces that this belief is held. No individual or organisation, outside the ARC membership is able to contribute, comment or provide feedback. Correspondence or questions around science are met with a stony silence. ARAN has not seen any cases where submissions from outside the ARC have been given any due consideration nor have ever resulted in change.
Prosecuting that the eminence of those supporting or promoting the view automatically means a position is true and above question – the ARC regards its internal consensus to be stronger that very low level evidence when formulating recommendations. Consensus is elevated to an inappropriate L.O.E. that out-ranks stronger levels of scientific evidence. This means change is slow and requires dis-proportionally high levels of evidence to change an opinion based on a very low, or low level scientific evidence. The ability to do this is reliant on a narcissistic belief in the gravitas of the individuals and the organisation i.e. infallibility by eminence. History has taught us that major advances are not the sole purvey of academics and researchers, but innovative disruptors that accelerate understanding and practice. This behaviour also inhibits a necessary dose of common sense from “interfering” with theoretically-based recommendations.
Work to ensure any interpretation of evidence showing a differing position is dismissed as irrelevant and excluded from review – the selective inclusion and exclusion of evidence was one of the prime mechanisms used by the Keys Hypothesis proponents to support an erroneous point of view for decades. The subjective formulation of consensus, especially in the face of poor evidence and then the elevation of that consensus to unquestionable truth is a hallmark of the ARC process of ensuring that their opinion is the sole and final accepted truth.
Treat any individual showing dissent from the excepted wisdom with ridicule and is defamed – Keys and his proponents found that one of the most effective techniques to quash alternate ideas was to attack the individual delivering these; to attempt to discredit and defame rather than argue from science. This strategy while unethical is exactly the tactic used to “manage” alternate ideas from those of the ARC. In practice this has included ARC actions such as, threatening legal action, attempting to damage businesses connected to an individual (thus threatening livelihood) and using their influence to bring frivolous and vexatious complaints to organisations that the individual is in a relationship with. Lastly, refusing to support external life-saving initiatives but then attempting to tear down and discredit those external initiatives that show promise or any chance of success.
Institute a policy whereby external enquiry in met with silence rather than science – given the actions in 4 above, the strategy of the ARC is to just simply not respond to questions, feedback or complaints; and certainly to treat all external correspondence as inferior and unworthy of consideration. This hubris goes on to treat their unethical actions as completely justified, conscionable and without accountability. Complaints are managed by ignoring them and attempting to punish the individual (as above) for the perceived audacity to assume that the organisation should be questioned. No response from external sources is ever met with a reasoned, evidence-based response; to the contrary they are curt, dismissive and lack any substance. It was not that long ago that access to all ARC material was restricted to only paying members. This seemed incongruous if the purpose was to save lives.
Establish yourself as “the authority”, the assumed source of “wisdom” and approval (with or without evidence) by regulatory means – once the Keys – Fat/Cholesterol = Heart Disease Hypothesis became part of government advice the assumption was made by all that this fact in itself proved that the hypothesis was in fact the ultimate truth. By becoming the source of “truth” Keys fulfilled in his own mind his true ambition of being seen as the father of modern population health. Despite the fact that populations following his advice continued to get fatter and heart disease rates continued to climb as cholesterol levels went down and fat consumption reduced; Keys stubbornly clung to his innate belief in his hypothesis or rather a hold on the “power” and respect he believed the scientific community and government had for him and his work. Likewise it is interesting to objectively look at the actual status of the ARC as an organisation vs. an authority which they claim as the infallible and sole purveyor of truth in regard to resuscitation in Australia. In itself the ARC has no inherent authority. It is after all a private, voluntary organisation. Its recommendations (as stated in on its own website) are merely the opinions of the individuals on the ARC and not the organisation of which they represent. There is no government oversight or accountability and not even formal representation by government in the decision making process. However, like Keys, the ARC has managed to establish itself as a monopoly on resuscitation advice, become the default reference source for government and industry and most importantly ensured that its opinions have been enshrined in regulations and policies as the de-facto authority on this subject. None of these achievements in themselves are proof that the opinions or consensus of the ARC are right or those recommendations in regard to practice work effectively or that they represent best-practice.
Restrict debate to those who accept the hypothesis or are sympathetic to it – the protection of the Keys Hypothesis extended to manipulating debate and scientific presentations on the subject of health and diet and to restrict the information going out to that which was sympathetic to Keys. The same strategy is used by the ARC to ensure only pro-consensus views are presented and discussed. Part of this strategy has already been mentioned already in refusing to debate science with anyone questioning their interpretation, the other is to influence thought and belief by restricting debate at conferences and forums by excluding any dissenting view from being aired. This has been demonstrated at not only their own “Spark of Life” conference where opposing views were rejected from the program but other events (including national and international functions) where the ARC has representation or influence over the organising committees. Whilst a lot of “back slapping” occurs at these events, there is no real forum for debate that threatens the ARC “authority” by questioning their accepted wisdom or processes.
Modify process to ensure the protection of opinion over science – one of the primary strategies employed by the ARC and Keys is and was to create a review process that excludes external oversight. Couple this with a policy that accepts no responsibility or accountability for the failure of its recommendation and practices. You have therefore a perfect storm for the creation and continuation of a private bureaucracy. A climate where even unproven methods can be forced upon the population or where old methods without efficacy can continue to be propagated as though they will be eternally correct. One would like to belief in the scientific community and especially the medical community that those in whom we entrust our health and well-being. Unfortunately, one can apply the quote below to both the history of the Keys Hypothesis and that of the ARC BLS/CPR Guidelines in Australia.
"In reality those that repudiate a theory that they once proposed or a theory that they accepted enthusiastically and with which they had identified themselves, are very rare. The great majority of them shut their ears so as not to hear the crying facts, and shut their eyes so as not to see the glaring facts, in order to remain faithful to their theories in spite of all and everything."
Maurice Arthur, Philosophy of Scientific Investigation ,1921
The process of forming consensus and making recommendations on practice may be flawed, however so is the process of ensuring currency, efficacy and accountability. The simple truth, the “pub test” if one prefers, is that if our current guidelines on BLS/CPR, etc. are superior and more evidence-based than other guidelines or approaches, firstly where is the evidence for this superiority and secondly we should be able to see measured, improved outcomes; the truth is that both of these are absent.
Moreover, the distance sometimes between consensus and the actual practice techniques and steps in guidelines is further evidence of a culture of belief that not only is the interpretation of science restricted to one group but that despite wider membership, guidelines are solely determined by individuals who do not actually work in nor understand the BLS area. As a result of this disconnect between consensus and practice, we see abdominal thrusts for FBAO rejected for a technique of one-handed chest thrust that have no relevant evidence or efficacy and don’t satisfy ILCOR’s own standards for inclusion; a population who is preparing itself for the most unlikely cardiac arrest possible, the hypoxic arrest in a healthy young person; impossible advice about chest compression depth that proposes a 7 year old child has the same chest depth as a 40 year old adult and a child in hypoglycemia being fed 10 Mentos without any understanding of the presence or absence of an effective gag reflex!
If the examples used in this paper related to an individual or a specific time period in history, then the reader may be tempted to disregard the behaviours outlines as “ancient history”, an “isolated case” or a “personal conflict”. However, there are many who (although too afraid of the consequences to their reputation and livelihood), have for many decades, been frustrated, disappointed and angry about the culture, attitudes and behaviour of the ARC.
What is the solution one may ask? ARAN has written about this previously, looking at the flawed consensus methodology, use of evidence and problems with governance. While these are tangible improvements the fundamental change that needs to take place is the self-perpetuating culture. I am not even sure if the majority of the hard-working members of the ARC (who are acting in good faith) understand or can see objectively what their organisation has become at an executive level and the type of questionable behaviours and practices their organisation is involved in and perpetuates. The other group that has to be considered are the partners of the ARC (under the ANZCOR banner), the New Zealand Resuscitation Council. They seem to be a body with integrity and an interest in practical measures over a political agenda. Their association with the ARC would seem a logical alliance, given the history of the two countries. However what they have inherited (not by choice) is the failings of their Australian counterparts and the negative impressions that the community has in Australia of the behaviours and attitudes of the ARC, including some less than ideal guideline recommendations. From my experience of the health sector in New Zealand, they generally are not disposed to follow Australia’s direction or solutions on anything automatically, but rather pragmatically consider practicalities and actual benefits before adopting anything; factors that override more political agendas in most cases.
It is apparent that the ARC can work with ILCOR and even has representation as a contributing body; however it seems the problems arise at the local level, where ILCOR consensus undergoes a re-consensus by local “experts” to formulate local recommendations and guidelines. This enables other agendas and politics to enter into the process and for outcomes to be ineffective, out of step with the international consensus or regimes that are just unworkable at (particularly) the public level. Local adaption could actually improve on ILCOR consensus (and resulting guidelines), but in Australia this unfortunately is rarely the case.
So what can we learn from the Keys/ARC comparison? There are some important lessons for individuals and organisations entrusted with the provision of advice for emergency situations just as for those who are trusted to give them the best advice on diet. Is it to do with the individuals? Of being physicians at the executive level? The problem Dotlich and Cairo (2003) list as narcissism-arrogance as the first (probably major cause) of why business leaders fail. They note four common symptoms:
1. A diminished capacity to learn from others or previous experience.
2. An off-putting outright refusal (ever) to be accountable and hence responsible.
3. Resistance to change because they know that ”their way” is best.
4. An inability to recognise their (manifold) limitations.
These behaviours seem familiar in both examples, Keys and the ARC. The difficulty is that the individuals (or group if this has metastasised to a culture) exhibiting these symptoms will by definition, not be able to recognise them and instead go on defending behaviours against what they would see as “unfair and unjustified criticism”.
ARAN
The current BLS Resuscitation Guidelines…
Is there authentic utility or just ensconced sciencism?
While there is an international scientific consensus on resuscitation, led by the International Liaison Committee on Resuscitation (ILCOR) publish treatment recommendations based on a review of the currently available literature via a GRADE methodology; each country who is a member of ILCOR (Australia included) formulates its own guidelines. These guidelines are ideally based on ILCOR treatment recommendations but also some local evidence review. In each case, the strength of the evidence is weighed to determine the final recommended practice. Most of this evidence (at both levels) falls into the “very low-quality evidence” categories and final recommendations and guidelines are therefore decided by discussion within reviewing panels, resulting in consensus opinion and practice recommendations.
In this methodology of “recommendations” and “guidelines”, practically all evidence is systematically eroded down to a very low quality and then the measures (of which there could be many that reflect the evidence) become emphatic recommendations (an oxymoron) and treated with the same reverence as fundamental laws of science. One could argue in fact, from a methodology perspective, that if the evidence is all of a “very poor” standard, then perhaps we are using the wrong measure. Apart from the central tenants of treatment many details of the actual methods (in BLS specifically) of achieving the recommendation (particularly at a local level) are not reviewed with the same scrutiny and many existing techniques and methodologies are assumed to be effective and sound without review. No experimentation or review of implementation efficacy is involved in the process and despite a very low-quality evidence base, no alternative solutions are considered in the system until they reach publication stage, with a tight definition of acceptable papers. Naturally, the further down the evidence tree a recommendations stem from the more likelihood that alternatives equally reflect the science as satisfactory remedies exist and the less dogmatic one can be of a single solution. This is well documented in the variance in end-user guidelines developed and available all based on the “same” consensus of evidence and treatment recommendations. It is quite evident that this consensus methodology, at least at the practical solutions end, may not always produce the best and most practical solution to satisfy the evidence nor definitively exclude variance. The process has limitation in an inability to take into account all circumstances, an inability to measure or test efficacy prior to the publication of a recommendation and an apparent inability to recognise and resolve resultant effects on other processes. The last limitation of this process is the loss of the ability to step back and (considering all the pieces) what does this mean to the average BLS provider? An obvious example is the treatment recommendations for a hypoglycaemic patient, where whilst on paper a Mentos may yield a more rapid effect in reversal, the Mentos is the perfect size to cause an airway obstruction, particularly in a patient with a diminished swallowing function. This guidance puts the recommendation at odds with choking-prevention advice (particularly in paediatric patients) and overlooks the advantages and common-sense of using alternate methods such as glucose gels (which incidentally the evidence review show similar result to that eventually recommended.
There is no intrinsic legislative or legal framework that enshrines these recommendations or guidelines as the only effective practice option and there is by the nature of the process an extended lag time in reviewing each new piece of evidence, either in measuring efficacy of recommendations and guidelines or research that may change these fundamentally. Unfortunately, processes like this often result in a cult-like following with zealots who mistakenly believe they are defending the ultimate “truth” of “scientism” and this is certainly the case in Australia. This in turn leads to a stifling of innovation and adaption at the coal face level (an important factor to adjust to circumstances and in the absence of resources) for fear of consequences that are just not present in non-professional care.
Notionally, in Australia the local representative body at ILCOR (the Australian Resuscitation Council - ARC), acknowledges that their guidance does not represent the only (or best) methods and techniques for “all situations” and further encourage implementers to seek advice on recommendations for differing circumstances. The first anomaly in Australia is that (by definition) the ARC cannot act as a reference source for differing methods and techniques for differing circumstance if the recommendations are dogmatically consistent to the point where difference is actively excluded despite a notional pledge to respect independence in practice.
In the absence of oversight or accountability and no accountability to consistency with already established, international consensus recommendations, there arises anomalies in local guidelines and treatment recommendations that either compound the “single remedy” limitations created by opinion at the international consensus or give way to local “re-consensus” to fit with opinion that may or may not reflect the science. Whilst the independence at the end-user level is notionally respected by all levels of the consensus process, how does one explain anomalies that exist, where the treatment recommendations of the ARC conflict with their own evidence review and/or the international treatment recommendations but still claim the same adherence to evidence directed care? More importantly why is this divergence considered “good science” sometimes and unnecessary on other occasions?
They are several examples (at a national level) that bear closer scrutiny in this review, where one may rightly struggle to differentiate the sometime arbitrary line where evidence and opinion (as competing factors) start and finish.
1. Compression only CPR and what “trained in ventilations” means
The recommendations and guidelines around the optimal CPR techniques for differing situations and circumstances have been clouded by two factors. The first is the conflation and confusion of variables in the evidence and secondly the political, unstated requisite for a single and all-encompassing piece of advice. These two factors have unquestionably (although not quantifiably) resulted in unnecessary deaths in cardiac arrest. One does not have to be a “rain man” to see that there are some discernible patterns amongst the available evidence and considerations.
Summation of what we know from the latest CoSTR statement from ILCOR and current AHA and ERC Guidelines.
The philosophy of population health (one would assume), is to enact the Latin phrase, “maxime bonum maxime populi” or the strategy of doing the “most good for most people”. The contradiction in the current focus of resuscitation is the methodology of preparation of the community for the exceptive case, so as to mitigate the risk of an emotive and unpopular oversight in actions.
2. Positioning of pregnant casualty during CPR:
The evidence, recommendations and resultant guidelines for this adaption is a confused and largely opinion-based measure. Comparing the evidence base, ILCOR recommendation, the ARC local review and the ARC Guidelines; one cannot come to the conclusion that the process has failed and has resulted in contradiction or Orwellian “double-think”.
“The maximum possible resuscitative force with chest compressions declines as the angle of inclination increases”
“There is no evidence re optimum position for chest compressions in pregnant women suffering cardiac arrest. In healthy pregnant women, there are conflicting results regarding effect of positioning on blood pressure, inferior vena cava diameter, cardiac output and central venous pressure. Although some studies presented in this review statistically significant differences, the clinical significance of many differences presented remains unclear. A review of evidence related to positioning in simulated cardiac arrest in pregnancy suggests a risk of decreased effectiveness of chest compressions when the ‘patient’ is placed in a lateral tilt position. In the absence of any strong evidence that lateral positioning improves haemodynamic parameters and the risk of lateral positioning resulting in reduced effectiveness of chest compressions, rescuers should continue to do what they know in terms of CPR (supine position, 30:2 compression to ventilation ratio) and not be distracted / impeded by the presence of pregnancy.”
It is quite apparent that the local guideline is neither based on the local evidence evaluation nor the ILCOR consensus. It is also apparent that the ambiguous nature of the remedy assumes each responder is equipped with a protractor and sufficient and appropriately shaped “towel” to accomplish this task. So as an exercise, let’s propose a measure that more closely addresses the evidence, a measure that used to be standard field practice for managing the issue of vena-cava compression during CPR. The technique, following gently moving the gravid uterus to the left is to keep it there by placing the patient’s own right hand/arm palm down under their own right buttock. So let us review how this technique reflects the available evidence:
Evidence and Consensus
3. The Management of Upper Airway Obstruction
If there is one subject that is evidence of where there is significant divergence of evidence interpretation and the influence of opinion and politics on recommendations, it is UAO. This subject is where Australia and New Zealand stand alone and in direct contrast to the consensus and evidence review of the entire international community. It is also an excellent example of where a supposedly rigorous and empirical system can result in contradictions and manipulations in the process of evidence evaluation to achieve a primarily political recommendation.
All international guidelines (other than ANZCOR), consensus and treatment recommendations recommend that FBAO in conscious patients over the age of 12 months; be managed using a combination of back blows (slaps), chest thrusts (carried out from behind the patient) and abdominal thrusts (Heimlich Manoeuvre or modified variant). There is no relevant or specific evidence that the alternative to abdominal thrusts used in the ANZCOR guidelines (chest thrust from in front of the patient) are effective or have resulted in any documented success.
ERC 2015 Guidelines - “A foreign body causing severe airway obstruction is a medical emergency and requires prompt treatment with back blows and, if that fails to relieve the obstruction, abdominal thrusts. If the victim becomes unresponsive CPR should be started immediately whilst help is summoned.” ARAN has already written extensively about the management of FBAO and the anomalies in the ARC Guidelines. Further information can be found on the site www.aran.org.au.
4. Hand Orientation during Compressions
Sometimes, recommendations and guidelines are punctuated with repeated images or descriptions of specific techniques that have not been as a result of a rigorous evidence review. In these instances, the reader can assume that a description (or illustration) of a component of a treatment recommendation is a condition of implementation without specific instruction. Hand orientation in compressions is a central example of this phenomenon. Without exception illustrations promulgate (by inference) the “interlocking fingers” technique of hand orientation as accepted “best-practice”.
The preference that the interlocking fingers technique is an appropriate, evidence-based technique is without evidence nor consideration by ILCOR or any other organisation. The history of the origin of this preferred technique comes clearly from the hypothesis that concentrating the force through one’s lower wrist and lifting the fingers from the chest would result in a decrease in the incidence of rib fractures during compressions. However, as all force is centralised it doubtful that this technique plays any role in the mitigation of rib fractures. Conversely, there is strong evidence for not using this technique for compressions. In 2013 the technique was tested bio-mechanically (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665060/), to establish the safety for users and the results clearly did not support this technique and rather concluded that:
“the forces transmitted through the rescuers’ wrists in the performance of external chest compressions during CPR are suffice to cause injury to the scapholunate ligament of the rescuer, potentially resulting in further cumulative trauma, degenerative changes, and eventual disability”
Further, that that forces required to rupture the ligament were in the order of 170N and typical compressions generated approximately 500N in the lower wrist (using the interlocking fingers technique). No consideration has been made of alternative methods to alleviate the significant wrist created by this inferred “best-practice”. There are several alternative techniques used by ambulance services around the world to alleviate this risk that have equal “evidence” and field assessment/evaluation that are more appropriate measures.
5. Depth of compression measurement
While the depth of compression is based on a review of evidence, the treatment recommendations (see example below from the ARC), is misleading in that it leads the reader to believe that the approximation of “1/3 of the chest depth” is equally based on evidence.
ARC – 2016 Guidelines
If the approximation of “1/3” was accurate is would by extrapolation mean that the reader must accept that for example a three (3) year old child has the same anatomical chest depth to a 50-year-old. By this reasoning, if 1/3 = 50mm in a child (over 1yo) and 1/3 of an adult = 51mm (>50mm) then the chest depth must be the same anatomically, otherwise the maths is very wrong.
The origins of this approximation are not clearly documented in the literature, however it’s likely origin is as an extrapolation from observations (only) of manikins during compressions, whereby typical compression manikins are a fraction of the chest depth (150-180mm vs. 230mm) of an actual patient and therefore a manikin 1/3 is a misleading observation.
6. Management of hypoglycaemia
The ILCOR treatment recommendation update on managing hypoglycaemic patients is an excellent example of where a scientific review process can fail to appropriately address future risk. This failing is primarily due to the absence of a risk management methodology i.e. that measures are analysed to assess their effectiveness in practice and whether in creating a measure, yet another risk is generated. While ANZCOR is in harmony with ILCOR in treatment recommendations on this issue (although historically recommendations can be divergent without evidence), this reflects blind compliance rather than this reflecting strength and solidarity of the process.
The current treatment recommendation updates state:
If the victim is able to follow simple commands and swallow safely, we recommend that first aid providers administer 15-20 grams glucose tablets (4 - 5 x 4 gram glucose tablets) for treatment of symptomatic hypoglycaemia [ILCOR CoSTR 2015 strong recommendation, low-quality evidence] 2,3,4, • If glucose tablets are not available, we suggest administering: • Confectionery including: o jelly beans (5-20 beans depending on the brand) o Skittles® (20-25 candies) o Mentos® (5-10 mints) [ILCOR CoSTR 2015, weak recommendation, very-low-quality evidence]2
Remembering that a “strong recommendation” just means it received general acceptance of opinion i.e. agreement based on very-low quality evidence does not make it a rigorous outcome. The logic of the scientific review process is that because there is insufficient evidence that safer techniques are more effective, and then a pragmatic decision to blindly rely on evidence alone (rather than risk) is the appropriate outcome.
7. Indicators for determining consciousness vs. unconsciousness
The accurate determination of “consciousness” is critical and pivotal piece of information in any BLS protocol. It signifies a potentially fatal condition, it determines the need for assistance and the need for further assessment of the patient is necessary to exclude the possibility of respiratory/cardio-respiratory arrest. Treatment recommendations in this area are far from having any evidence to support the “stance” taken in guidelines by individual countries. Historically (and still in use in the UK), the method in BLS of determining the conscious status was referred to a “shake and shout” i.e. shake the shoulders and shout at the patient to determine a “response”. For many years (particularly in Australia), guidelines have reflected a more liberal and sensitive notion involving the use of “gentle shoulder squeezes and to ask a question of the casualty”. From a neurological perspective, these relatively new methods (especially) cannot by definition establish “consciousness” and are at best an assessment of sleeping state.
These changes were made to provide perhaps a “safer” assessment (given a very small risk of spinal injury), however for the most part, these new indicators are merely a result of a “politically correct” focus over effectiveness. The difficulties with the efficacy of this recommendation are rooted in a simple but inescapable truth i.e. that gently squeezing the shoulders and politely asking a question, are not and never have been clinical indicators of consciousness/unconsciousness. The fact that this assessment is happening in BLS (with no pulse checks and little experience and training) does not justify a lack of effectiveness and increasing ambiguity of the patient’s condition. These two modern day approaches never have been and will never be clinical indicators of consciousness/unconsciousness. Let us image for a moment that we were working in an Intensive Care Unit (ICU) and we were tasked with doing regular neuro-observations on unconscious and ventilated patients. To wit, we wrote on the patient notes that we have “squeezed their shoulders gently and whispered positive affirmations into their ear” and concluded they were “unconscious”. Our career in ICU would probably last less than 5 minutes, as we have not used bona-fide clinical indicators, but rather chose to make up some alternatives as the basis of our clinical treatment. Non-response to verbal commands and gentle touch may be appropriate in assessing “reusability” in sleep but not confirming unconsciousness.
Ultimately, the only appropriate differential diagnosis of “unconsciousness” in BLS primary assessment is the patient’s response to painful stimuli. This may is the patient’s response to painful stimuli. This may at the conclusion of an escalating assessment i.e. beginning with voice commands and touch, however it must conclude (in the absence of a response) to a pain assessment. Doing otherwise and basing the subsequent actions on poor and inappropriate techniques has no basis in clinical practice or scientific evidence. There are several methods of pain assessment that can be used by BLS providers that are safe and will not cause injury or liability; however, they will provide a more accurate assessment of the status of the patient and more accurately determine subsequent actions. “Sternal Rubs”, pressure on the nail beds with the thumb nail for example or pulling in the hairs on the arms and legs; are all safe and accurate determinations for the BLS provider.
The other determinate of “consciousness” in BLS is the absence of “normal breathing”. While acknowledging that the mere presence or absence of breathing function is not an accurate measure (given that 35-55% of all cardiac arrest patients will initially present with agonal respirations) the description defining “normal” vs “abnormal” is ill defined and is a significant factor in the delay of resuscitation and the misdiagnosis of cardiac arrest. This “abnormal” breathing function does not include slow (but regular breathing) being the most common description non-professionals have of what is in fact, normal breathing. The description of agonal respirations is best summarised as “gasps and/or sighs, punctuated by long periods of silence (with or without apparent air movement)”.
8. Airway management recommendations in BLS
Another anomaly with BLS recommendations and subsequent guidelines is the inconsistent trust in the aptitude of BLS (non-professional) providers, who have limited training and often no experience. Some recommendations and guidelines assume that BLS have an ability to appropriately and accurately determine indicators, such as the presence of agonal respirations as equivalent to “no respirations” or the ability to ventilate patients after rudimentary training (without causing gastric distention and aspiration)and then in other recommendations and guideline there is a underlying mistrust of the ability and skills of BLS providers e.g. that they are incapable of any other airway management method than “head-tilt” over a more widely applicable technique (in the typical cardiac arrest) of “jaw thrust”. Jaw thrust is clearly more effective on the more typical cardiac arrest patient, including: obese patients (where neck fat tissue and larger “floppy” pallets make for common obstructions beyond the help of simple head tilt); suspected cervical spinal injury; infants; Down’s Syndrome patients; patients with degenerative spinal conditions or previous cervical previous and patients with advanced osteoarthritis with pronounced kyphosis of the neck. As these are more common presentations in cardiac arrest than the stylised young, healthy child/adolescent it would seem anomalous that “head tilt” would be preferred in BLS. Training in the head tilt manoeuvre is no more complex or difficult that current head tilt/chin lift processes, however the two are seen as mutually exclusive in BLS vs. ALS.
9.Is the DRSABCD – too general to be universally useful?
Whilst the evidence is very clear that most cardiac arrests (>80%) are of Sudden Cardiac Arrests (SCA’s), there is a orthodoxy around BLS guidelines that attempts to cover all aetiologies with a singular, simplistic and indiscriminate “action plan”. This approach (which implies that hypoxia aetiologies are the common presentation rather than the exception to the rule) does little justice to the actuality of events and biases response toward methodologies that produce poorer results for the majority to mitigate the possible risk of misdiagnosing the rare event.
Shortcomings of this orthodox approach mean that the effective measures, such as fast/deep compressions and early defibrillation are relegated to less critical (and evidence-based) to measures such as airway clearance and ventilation in SCA. In emergency scenes with perhaps multiple casualties, the DRSABCD approach does not address the priorities of a “scene” over those of an individual patient and in minor BLS (First Aid) situations it is substantially redundant. As already highlighted the existing regime bases decisions on two ambiguous and/or ineffective measures in BLS i.e. consciousness assessment without reference to painful stimuli and the assessment of “normal breathing”.
Essentially, the “status-quo”, prioritises actions based on likely aetiology of the arrest as a singular, common regime regardless of the cause or presence of a non-collapse scenario.
The evidence is conclusive and should drive changes to this “status quo” to address the differences in treatment values:
It is apparent and despite good intentions, just because all the actions in the DRSABCD may play a part in survival (in some circumstance), does not necessarily mean all arrest aetiologies need each step similarly nor that the steps are in the optimal order for all situations. It is also very apparent that the science of resuscitation is very much pointing toward the failure of the singular protocol treatment methodology. As an example, in separating a traumatic BLS response protocol from a “collapse” protocol for bystanders (this includes those with rudimentary training in CPR e.g. a BLS/CPR course); a protocol may follow a much simpler set of core elements and decision point’s i.e.:
(If the answer is YES to one or both of these questions the patient does not need resuscitation. Look for other causes).
If the answer is NO to both these questions start fast, deep chest compression immediately and send someone to retrieve AED and send for medical/emergency assistance e.g. 000 or medical response in health facilities.
In the present DRSABCD, only partial (or ineffective versions) of these elements are present. While it might be argued that the additional elements are provided through training (i.e. that the DRSABCD is a promoting framework) the reality for the non-professional is that the existing protocol is usual. While it might be argued that the additional elements are provided through training the reality for the non-professional is that any detail of the existing protocol is usually forgotten in both simulated and actual emergencies.
Conclusions
The goal of simplicity i.e. to provide the “lowliest” devotee with an unambiguous plan of action is not without merit, however the application of this plan of action in BLS has been for too long riddled with ambiguities, compromises and a lack of necessary discernment. One could easily conclude in even a brief examination of the detail that “common sense” and an appreciation of the realities of the application of BLS, still do not feature strongly in resultant guidelines.
This situation has resulted (and is perpetuated) by several factors. These include: that the intrinsic inertia generated from the notion that fundamental changes will confuse more than improve outcomes; that BLS providers are incapable of anything more but will be more effective with a narrower scope of practice; that without pre-requisite experimentation and accountability in guideline implementation there is no sound evidence that hypothesis based on interpretation of evidence with necessarily result in the best and most practice treatment recommendations; that there is a local culture in evidence interpretation that gives rise to (and is presented as) a presumption of unquestionable, accepted dogma; that the treatment recommendation devised by one group (expert or not) based on an interpretation of evidence (a consensus) may not be the only, best, safest or most easily translated into action at user level, recommendation available; that the elevation of treatment recommendations and guidelines (based on restrictive and purely theoretical consensus) to the status of “scientific law” is not scientific; that the methodologies of evidence review that relegates the field of BLS resuscitation practice to being largely based on “poor or very week evidence” is a flawed and inappropriate methodology for this field of science; that despite a claim of strong scientific rigour, resuscitation recommendations are also governed by the same political factors that have corrupted public understanding, acceptance and revelation of truth as every other area of science and this has led to some treatment recommendations that have become canon and are unable to be changed in the face of evidence or simple ambiguity or lack of utility.
If it were possible to remove the other, (non-patient outcome focused) factors from resuscitation guidelines and treatment recommendations, what indeed would the landscape look like? The conclusion raised in this paper is both straightforward and challenging i.e. If long-standing ambiguities are able to still be readily identified in continuing and newly implemented regimes, then the system governing and maintaining these regimes is significantly flawed and misguided. These anomalies are easily identified by anyone who makes more than a cursory review of treatment recommendations and guidelines and serve only to undermine both the methodology used and the factual and established framework.
At the BLS level there are several factors borne out from experience and the evidence:
The methodology used to develop local guidelines is founded on the notion that all Australian guidelines are “agreed to” by all stakeholders and therefore represent accepted “best practice” is fundamentally flawed and disingenuous. The only decision makers for the determination of content and structure of local guidelines sit at the top of a bureaucratic pyramid. As guidelines are viewed as “edicts from on high” there is little resistance at lower levels and any contrary view or call for change, has no power to affect change against an “expert hierarchy” and is actively dismissed and resisted.
Sciencism and a lack of true utility have been the result of this system as seen by these examples in this paper, however this is not exhaustive. It can be seen that the value of current treatment recommendations and guidelines cannot be accepted on face value alone as although resulting from a formal consensus process, this does not guarantee utility nor that they are any more than opinions based on poor science and entrenched sciencism. Re-enforcing established simplistic (and stylised) treatment recommendations and guidelines, in the absence of evidence of utility cannot realise the quality of outcomes that are possible. The 2017 ILCOR Summary Statement identifies a plethora of fundamental knowledge gaps in CPR practice (summarised down to no less than 18 in the ILCOR document); knowledge gaps that undermine any attempt to formulate credible recommendations, that can be so commonly followed without question.
References
ILCOR Knowledge Gaps and Clinical Research Priorities for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, Circulation 2018
Australian Resuscitation Council Guideline 6 – Compressions, Evidence Worksheet
Australian Resuscitation Council Guideline 6 – Compressions
Australian Resuscitation Council Guideline 9.2.9 – First aid Management of a Diabetic Emergency
2017 International Consensus on Cardiopulmonary Resuscitation and emergency Cardiovascular Care Science with Treatment Recommendations Summary, 2017 ERC and AHA
Minimally Interrupted Cardiac resuscitation by Emergency Medical Services for Out-of-Hospital Cardiac Arrest Bentley J. Bobrow, MD Lani L. Clark, BS Gordon A. Ewy, MD Vatsal Chikani, MPH Arthur B. Sanders, MD Robert A. Berg, MD Peter B. Richman, MD Karl B. Kern, MD, JAMA, March 12, 2008—Vol 299, No. 10
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665060/
Is there authentic utility or just ensconced sciencism?
While there is an international scientific consensus on resuscitation, led by the International Liaison Committee on Resuscitation (ILCOR) publish treatment recommendations based on a review of the currently available literature via a GRADE methodology; each country who is a member of ILCOR (Australia included) formulates its own guidelines. These guidelines are ideally based on ILCOR treatment recommendations but also some local evidence review. In each case, the strength of the evidence is weighed to determine the final recommended practice. Most of this evidence (at both levels) falls into the “very low-quality evidence” categories and final recommendations and guidelines are therefore decided by discussion within reviewing panels, resulting in consensus opinion and practice recommendations.
In this methodology of “recommendations” and “guidelines”, practically all evidence is systematically eroded down to a very low quality and then the measures (of which there could be many that reflect the evidence) become emphatic recommendations (an oxymoron) and treated with the same reverence as fundamental laws of science. One could argue in fact, from a methodology perspective, that if the evidence is all of a “very poor” standard, then perhaps we are using the wrong measure. Apart from the central tenants of treatment many details of the actual methods (in BLS specifically) of achieving the recommendation (particularly at a local level) are not reviewed with the same scrutiny and many existing techniques and methodologies are assumed to be effective and sound without review. No experimentation or review of implementation efficacy is involved in the process and despite a very low-quality evidence base, no alternative solutions are considered in the system until they reach publication stage, with a tight definition of acceptable papers. Naturally, the further down the evidence tree a recommendations stem from the more likelihood that alternatives equally reflect the science as satisfactory remedies exist and the less dogmatic one can be of a single solution. This is well documented in the variance in end-user guidelines developed and available all based on the “same” consensus of evidence and treatment recommendations. It is quite evident that this consensus methodology, at least at the practical solutions end, may not always produce the best and most practical solution to satisfy the evidence nor definitively exclude variance. The process has limitation in an inability to take into account all circumstances, an inability to measure or test efficacy prior to the publication of a recommendation and an apparent inability to recognise and resolve resultant effects on other processes. The last limitation of this process is the loss of the ability to step back and (considering all the pieces) what does this mean to the average BLS provider? An obvious example is the treatment recommendations for a hypoglycaemic patient, where whilst on paper a Mentos may yield a more rapid effect in reversal, the Mentos is the perfect size to cause an airway obstruction, particularly in a patient with a diminished swallowing function. This guidance puts the recommendation at odds with choking-prevention advice (particularly in paediatric patients) and overlooks the advantages and common-sense of using alternate methods such as glucose gels (which incidentally the evidence review show similar result to that eventually recommended.
There is no intrinsic legislative or legal framework that enshrines these recommendations or guidelines as the only effective practice option and there is by the nature of the process an extended lag time in reviewing each new piece of evidence, either in measuring efficacy of recommendations and guidelines or research that may change these fundamentally. Unfortunately, processes like this often result in a cult-like following with zealots who mistakenly believe they are defending the ultimate “truth” of “scientism” and this is certainly the case in Australia. This in turn leads to a stifling of innovation and adaption at the coal face level (an important factor to adjust to circumstances and in the absence of resources) for fear of consequences that are just not present in non-professional care.
Notionally, in Australia the local representative body at ILCOR (the Australian Resuscitation Council - ARC), acknowledges that their guidance does not represent the only (or best) methods and techniques for “all situations” and further encourage implementers to seek advice on recommendations for differing circumstances. The first anomaly in Australia is that (by definition) the ARC cannot act as a reference source for differing methods and techniques for differing circumstance if the recommendations are dogmatically consistent to the point where difference is actively excluded despite a notional pledge to respect independence in practice.
In the absence of oversight or accountability and no accountability to consistency with already established, international consensus recommendations, there arises anomalies in local guidelines and treatment recommendations that either compound the “single remedy” limitations created by opinion at the international consensus or give way to local “re-consensus” to fit with opinion that may or may not reflect the science. Whilst the independence at the end-user level is notionally respected by all levels of the consensus process, how does one explain anomalies that exist, where the treatment recommendations of the ARC conflict with their own evidence review and/or the international treatment recommendations but still claim the same adherence to evidence directed care? More importantly why is this divergence considered “good science” sometimes and unnecessary on other occasions?
They are several examples (at a national level) that bear closer scrutiny in this review, where one may rightly struggle to differentiate the sometime arbitrary line where evidence and opinion (as competing factors) start and finish.
- Compression only CPR and what “trained in ventilations” means
- Positioning of the pregnant patient during CPR
- The management of Upper Airway Obstruction
- Hand orientation for CPR compressions
- Depth of compression recommendations
- Management of hypoglycaemia
- Indicators for determining unconsciousness
- Airway management recommendations in BLS
- Is the DRSABCD – still relevant in BLS?
1. Compression only CPR and what “trained in ventilations” means
The recommendations and guidelines around the optimal CPR techniques for differing situations and circumstances have been clouded by two factors. The first is the conflation and confusion of variables in the evidence and secondly the political, unstated requisite for a single and all-encompassing piece of advice. These two factors have unquestionably (although not quantifiably) resulted in unnecessary deaths in cardiac arrest. One does not have to be a “rain man” to see that there are some discernible patterns amongst the available evidence and considerations.
Summation of what we know from the latest CoSTR statement from ILCOR and current AHA and ERC Guidelines.
- SCA is a significant public health issue and while rates vary between countries, it is by far (by an enormous magnitude) the most common aetiology of cardiac arrest. Cardiac arrest from hypoxic and traumatic aetiologies, probably need to be managed as exceptions.
- Dispatcher assisted CPR (non-clinical call-takers in Australia) should be “compressions only”.
- Bystanders and non-clinical Ambulance call-takers are not reliably or effectively able to determine the presence of “agonal respirations” in cardiac arrest.
- The ability (and benefit) of basically “trained” bystanders to deliver ventilations is not established.
- Initial minimal ventilation (even passive) provides better outcomes in SCA.
- A period of “compressions only” CPR by emergency personnel shows improved outcomes in SCA (witnessed).
- Skills decay in minimally trained bystanders can occur very quickly.
- Jaw thrust whilst more effective and more widely applicable to the “typical” cardiac arrest scenario is not recommended as a necessary skill in BLS as it is assumed to be “difficult to learn” (opinion by ILCOR with no evidence). However, ignorance of this technique further compounds the risks associated with BLS ventilations.
- In SCA there are only 3 measures with sufficient evidence to be bystander BLS appropriate (this includes minimally “trained” individuals i.e. current BLS CPR) Œ Call for help Commence fast and deep compressions with full recoil Ž Early Defibrillation (preferably in <3 mins not > 5 minutes from time of collapse).
- The optimum sequence for BLS is unknown but is probably dependant on aetiology of the arrest and clinical quality of the response. In is evident that initial defibrillation and constant compressions should not be delayed in deference to other non-evidenced interventions in BLS e.g. airway management and ventilations.
The philosophy of population health (one would assume), is to enact the Latin phrase, “maxime bonum maxime populi” or the strategy of doing the “most good for most people”. The contradiction in the current focus of resuscitation is the methodology of preparation of the community for the exceptive case, so as to mitigate the risk of an emotive and unpopular oversight in actions.
2. Positioning of pregnant casualty during CPR:
The evidence, recommendations and resultant guidelines for this adaption is a confused and largely opinion-based measure. Comparing the evidence base, ILCOR recommendation, the ARC local review and the ARC Guidelines; one cannot come to the conclusion that the process has failed and has resulted in contradiction or Orwellian “double-think”.
- ILCOR CoSTR 2015 –
- ERC Consensus - 2017
- ARC Worksheet of Evidence supporting 2016 Guidelines –
“The maximum possible resuscitative force with chest compressions declines as the angle of inclination increases”
“There is no evidence re optimum position for chest compressions in pregnant women suffering cardiac arrest. In healthy pregnant women, there are conflicting results regarding effect of positioning on blood pressure, inferior vena cava diameter, cardiac output and central venous pressure. Although some studies presented in this review statistically significant differences, the clinical significance of many differences presented remains unclear. A review of evidence related to positioning in simulated cardiac arrest in pregnancy suggests a risk of decreased effectiveness of chest compressions when the ‘patient’ is placed in a lateral tilt position. In the absence of any strong evidence that lateral positioning improves haemodynamic parameters and the risk of lateral positioning resulting in reduced effectiveness of chest compressions, rescuers should continue to do what they know in terms of CPR (supine position, 30:2 compression to ventilation ratio) and not be distracted / impeded by the presence of pregnancy.”
- ANZCOR Guideline 6 Compressions Jan 2016 –
It is quite apparent that the local guideline is neither based on the local evidence evaluation nor the ILCOR consensus. It is also apparent that the ambiguous nature of the remedy assumes each responder is equipped with a protractor and sufficient and appropriately shaped “towel” to accomplish this task. So as an exercise, let’s propose a measure that more closely addresses the evidence, a measure that used to be standard field practice for managing the issue of vena-cava compression during CPR. The technique, following gently moving the gravid uterus to the left is to keep it there by placing the patient’s own right hand/arm palm down under their own right buttock. So let us review how this technique reflects the available evidence:
Evidence and Consensus
- “Even a small amount of tilt may be better than no tilt. The angle of tilt used needs to enable high-quality chest compressions and if needed.”
- “Decreased effectiveness of chest compressions when the ‘patient’ is placed in a lateral tilt position.”
- “Add left lateral tilt if this is feasible and ensure the chest remains supported on a firm surface – the optimal angle of tilt is unknown”
- “The maximum possible resuscitative force with chest compressions declines as the angle of inclination increases”
3. The Management of Upper Airway Obstruction
If there is one subject that is evidence of where there is significant divergence of evidence interpretation and the influence of opinion and politics on recommendations, it is UAO. This subject is where Australia and New Zealand stand alone and in direct contrast to the consensus and evidence review of the entire international community. It is also an excellent example of where a supposedly rigorous and empirical system can result in contradictions and manipulations in the process of evidence evaluation to achieve a primarily political recommendation.
All international guidelines (other than ANZCOR), consensus and treatment recommendations recommend that FBAO in conscious patients over the age of 12 months; be managed using a combination of back blows (slaps), chest thrusts (carried out from behind the patient) and abdominal thrusts (Heimlich Manoeuvre or modified variant). There is no relevant or specific evidence that the alternative to abdominal thrusts used in the ANZCOR guidelines (chest thrust from in front of the patient) are effective or have resulted in any documented success.
ERC 2015 Guidelines - “A foreign body causing severe airway obstruction is a medical emergency and requires prompt treatment with back blows and, if that fails to relieve the obstruction, abdominal thrusts. If the victim becomes unresponsive CPR should be started immediately whilst help is summoned.” ARAN has already written extensively about the management of FBAO and the anomalies in the ARC Guidelines. Further information can be found on the site www.aran.org.au.
4. Hand Orientation during Compressions
Sometimes, recommendations and guidelines are punctuated with repeated images or descriptions of specific techniques that have not been as a result of a rigorous evidence review. In these instances, the reader can assume that a description (or illustration) of a component of a treatment recommendation is a condition of implementation without specific instruction. Hand orientation in compressions is a central example of this phenomenon. Without exception illustrations promulgate (by inference) the “interlocking fingers” technique of hand orientation as accepted “best-practice”.
The preference that the interlocking fingers technique is an appropriate, evidence-based technique is without evidence nor consideration by ILCOR or any other organisation. The history of the origin of this preferred technique comes clearly from the hypothesis that concentrating the force through one’s lower wrist and lifting the fingers from the chest would result in a decrease in the incidence of rib fractures during compressions. However, as all force is centralised it doubtful that this technique plays any role in the mitigation of rib fractures. Conversely, there is strong evidence for not using this technique for compressions. In 2013 the technique was tested bio-mechanically (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665060/), to establish the safety for users and the results clearly did not support this technique and rather concluded that:
“the forces transmitted through the rescuers’ wrists in the performance of external chest compressions during CPR are suffice to cause injury to the scapholunate ligament of the rescuer, potentially resulting in further cumulative trauma, degenerative changes, and eventual disability”
Further, that that forces required to rupture the ligament were in the order of 170N and typical compressions generated approximately 500N in the lower wrist (using the interlocking fingers technique). No consideration has been made of alternative methods to alleviate the significant wrist created by this inferred “best-practice”. There are several alternative techniques used by ambulance services around the world to alleviate this risk that have equal “evidence” and field assessment/evaluation that are more appropriate measures.
5. Depth of compression measurement
While the depth of compression is based on a review of evidence, the treatment recommendations (see example below from the ARC), is misleading in that it leads the reader to believe that the approximation of “1/3 of the chest depth” is equally based on evidence.
ARC – 2016 Guidelines
If the approximation of “1/3” was accurate is would by extrapolation mean that the reader must accept that for example a three (3) year old child has the same anatomical chest depth to a 50-year-old. By this reasoning, if 1/3 = 50mm in a child (over 1yo) and 1/3 of an adult = 51mm (>50mm) then the chest depth must be the same anatomically, otherwise the maths is very wrong.
The origins of this approximation are not clearly documented in the literature, however it’s likely origin is as an extrapolation from observations (only) of manikins during compressions, whereby typical compression manikins are a fraction of the chest depth (150-180mm vs. 230mm) of an actual patient and therefore a manikin 1/3 is a misleading observation.
6. Management of hypoglycaemia
The ILCOR treatment recommendation update on managing hypoglycaemic patients is an excellent example of where a scientific review process can fail to appropriately address future risk. This failing is primarily due to the absence of a risk management methodology i.e. that measures are analysed to assess their effectiveness in practice and whether in creating a measure, yet another risk is generated. While ANZCOR is in harmony with ILCOR in treatment recommendations on this issue (although historically recommendations can be divergent without evidence), this reflects blind compliance rather than this reflecting strength and solidarity of the process.
The current treatment recommendation updates state:
If the victim is able to follow simple commands and swallow safely, we recommend that first aid providers administer 15-20 grams glucose tablets (4 - 5 x 4 gram glucose tablets) for treatment of symptomatic hypoglycaemia [ILCOR CoSTR 2015 strong recommendation, low-quality evidence] 2,3,4, • If glucose tablets are not available, we suggest administering: • Confectionery including: o jelly beans (5-20 beans depending on the brand) o Skittles® (20-25 candies) o Mentos® (5-10 mints) [ILCOR CoSTR 2015, weak recommendation, very-low-quality evidence]2
Remembering that a “strong recommendation” just means it received general acceptance of opinion i.e. agreement based on very-low quality evidence does not make it a rigorous outcome. The logic of the scientific review process is that because there is insufficient evidence that safer techniques are more effective, and then a pragmatic decision to blindly rely on evidence alone (rather than risk) is the appropriate outcome.
7. Indicators for determining consciousness vs. unconsciousness
The accurate determination of “consciousness” is critical and pivotal piece of information in any BLS protocol. It signifies a potentially fatal condition, it determines the need for assistance and the need for further assessment of the patient is necessary to exclude the possibility of respiratory/cardio-respiratory arrest. Treatment recommendations in this area are far from having any evidence to support the “stance” taken in guidelines by individual countries. Historically (and still in use in the UK), the method in BLS of determining the conscious status was referred to a “shake and shout” i.e. shake the shoulders and shout at the patient to determine a “response”. For many years (particularly in Australia), guidelines have reflected a more liberal and sensitive notion involving the use of “gentle shoulder squeezes and to ask a question of the casualty”. From a neurological perspective, these relatively new methods (especially) cannot by definition establish “consciousness” and are at best an assessment of sleeping state.
These changes were made to provide perhaps a “safer” assessment (given a very small risk of spinal injury), however for the most part, these new indicators are merely a result of a “politically correct” focus over effectiveness. The difficulties with the efficacy of this recommendation are rooted in a simple but inescapable truth i.e. that gently squeezing the shoulders and politely asking a question, are not and never have been clinical indicators of consciousness/unconsciousness. The fact that this assessment is happening in BLS (with no pulse checks and little experience and training) does not justify a lack of effectiveness and increasing ambiguity of the patient’s condition. These two modern day approaches never have been and will never be clinical indicators of consciousness/unconsciousness. Let us image for a moment that we were working in an Intensive Care Unit (ICU) and we were tasked with doing regular neuro-observations on unconscious and ventilated patients. To wit, we wrote on the patient notes that we have “squeezed their shoulders gently and whispered positive affirmations into their ear” and concluded they were “unconscious”. Our career in ICU would probably last less than 5 minutes, as we have not used bona-fide clinical indicators, but rather chose to make up some alternatives as the basis of our clinical treatment. Non-response to verbal commands and gentle touch may be appropriate in assessing “reusability” in sleep but not confirming unconsciousness.
Ultimately, the only appropriate differential diagnosis of “unconsciousness” in BLS primary assessment is the patient’s response to painful stimuli. This may is the patient’s response to painful stimuli. This may at the conclusion of an escalating assessment i.e. beginning with voice commands and touch, however it must conclude (in the absence of a response) to a pain assessment. Doing otherwise and basing the subsequent actions on poor and inappropriate techniques has no basis in clinical practice or scientific evidence. There are several methods of pain assessment that can be used by BLS providers that are safe and will not cause injury or liability; however, they will provide a more accurate assessment of the status of the patient and more accurately determine subsequent actions. “Sternal Rubs”, pressure on the nail beds with the thumb nail for example or pulling in the hairs on the arms and legs; are all safe and accurate determinations for the BLS provider.
The other determinate of “consciousness” in BLS is the absence of “normal breathing”. While acknowledging that the mere presence or absence of breathing function is not an accurate measure (given that 35-55% of all cardiac arrest patients will initially present with agonal respirations) the description defining “normal” vs “abnormal” is ill defined and is a significant factor in the delay of resuscitation and the misdiagnosis of cardiac arrest. This “abnormal” breathing function does not include slow (but regular breathing) being the most common description non-professionals have of what is in fact, normal breathing. The description of agonal respirations is best summarised as “gasps and/or sighs, punctuated by long periods of silence (with or without apparent air movement)”.
8. Airway management recommendations in BLS
Another anomaly with BLS recommendations and subsequent guidelines is the inconsistent trust in the aptitude of BLS (non-professional) providers, who have limited training and often no experience. Some recommendations and guidelines assume that BLS have an ability to appropriately and accurately determine indicators, such as the presence of agonal respirations as equivalent to “no respirations” or the ability to ventilate patients after rudimentary training (without causing gastric distention and aspiration)and then in other recommendations and guideline there is a underlying mistrust of the ability and skills of BLS providers e.g. that they are incapable of any other airway management method than “head-tilt” over a more widely applicable technique (in the typical cardiac arrest) of “jaw thrust”. Jaw thrust is clearly more effective on the more typical cardiac arrest patient, including: obese patients (where neck fat tissue and larger “floppy” pallets make for common obstructions beyond the help of simple head tilt); suspected cervical spinal injury; infants; Down’s Syndrome patients; patients with degenerative spinal conditions or previous cervical previous and patients with advanced osteoarthritis with pronounced kyphosis of the neck. As these are more common presentations in cardiac arrest than the stylised young, healthy child/adolescent it would seem anomalous that “head tilt” would be preferred in BLS. Training in the head tilt manoeuvre is no more complex or difficult that current head tilt/chin lift processes, however the two are seen as mutually exclusive in BLS vs. ALS.
9.Is the DRSABCD – too general to be universally useful?
Whilst the evidence is very clear that most cardiac arrests (>80%) are of Sudden Cardiac Arrests (SCA’s), there is a orthodoxy around BLS guidelines that attempts to cover all aetiologies with a singular, simplistic and indiscriminate “action plan”. This approach (which implies that hypoxia aetiologies are the common presentation rather than the exception to the rule) does little justice to the actuality of events and biases response toward methodologies that produce poorer results for the majority to mitigate the possible risk of misdiagnosing the rare event.
Shortcomings of this orthodox approach mean that the effective measures, such as fast/deep compressions and early defibrillation are relegated to less critical (and evidence-based) to measures such as airway clearance and ventilation in SCA. In emergency scenes with perhaps multiple casualties, the DRSABCD approach does not address the priorities of a “scene” over those of an individual patient and in minor BLS (First Aid) situations it is substantially redundant. As already highlighted the existing regime bases decisions on two ambiguous and/or ineffective measures in BLS i.e. consciousness assessment without reference to painful stimuli and the assessment of “normal breathing”.
Essentially, the “status-quo”, prioritises actions based on likely aetiology of the arrest as a singular, common regime regardless of the cause or presence of a non-collapse scenario.
The evidence is conclusive and should drive changes to this “status quo” to address the differences in treatment values:
- Most (>80%) of all OHCA’s are of SCA’s type.
- Approximately 80-85% of all SCA’s will develop a “shockable” rhythm (VF/VT) in the first 8-9 minutes.
- In SCA there are only 3 measures in the initial few minutes (pre-ambulance (LS) phase that are pivotal to both short and long-term survival:
- Seek help
- Commence fast, deep chest compressions
- Defibrillate as soon as possible (<3 mins but no more than 5 mins)
- Outside the initial 6 minutes, the application of ALS will have minimal impact on long term outcome in SCA.
- Hypoxic and traumatic aetiology are minor causes of OHCA.
- Ventilations in BLS may only be beneficial in unwitnessed SCA and Hypoxic arrests.
It is apparent and despite good intentions, just because all the actions in the DRSABCD may play a part in survival (in some circumstance), does not necessarily mean all arrest aetiologies need each step similarly nor that the steps are in the optimal order for all situations. It is also very apparent that the science of resuscitation is very much pointing toward the failure of the singular protocol treatment methodology. As an example, in separating a traumatic BLS response protocol from a “collapse” protocol for bystanders (this includes those with rudimentary training in CPR e.g. a BLS/CPR course); a protocol may follow a much simpler set of core elements and decision point’s i.e.:
- On approach, assess for any hazards and call for bystander assistance
- At the patient, establish if the patient is?
- Responsive to pain?
- Breathing normally?
(If the answer is YES to one or both of these questions the patient does not need resuscitation. Look for other causes).
If the answer is NO to both these questions start fast, deep chest compression immediately and send someone to retrieve AED and send for medical/emergency assistance e.g. 000 or medical response in health facilities.
- If resuscitation is indicated switch on the AED and follow prompts
- When the emergency staff equipment arrives, they will make decisions about airway management, ventilation and the need for further assistance. If medical assistance is delayed (>6 minutes from collapse) in in cases of paediatric or drowning aetiology, consider ventilation.
- Assess the scene for hazards
- Assess the scope the situation, including number and location of casualties.
- Decide and summon help on-hand and help required.
- Prioritise treatment need of casualties.
- Detailed assessment of individual casualties as required and treatment.
In the present DRSABCD, only partial (or ineffective versions) of these elements are present. While it might be argued that the additional elements are provided through training (i.e. that the DRSABCD is a promoting framework) the reality for the non-professional is that the existing protocol is usual. While it might be argued that the additional elements are provided through training the reality for the non-professional is that any detail of the existing protocol is usually forgotten in both simulated and actual emergencies.
Conclusions
The goal of simplicity i.e. to provide the “lowliest” devotee with an unambiguous plan of action is not without merit, however the application of this plan of action in BLS has been for too long riddled with ambiguities, compromises and a lack of necessary discernment. One could easily conclude in even a brief examination of the detail that “common sense” and an appreciation of the realities of the application of BLS, still do not feature strongly in resultant guidelines.
This situation has resulted (and is perpetuated) by several factors. These include: that the intrinsic inertia generated from the notion that fundamental changes will confuse more than improve outcomes; that BLS providers are incapable of anything more but will be more effective with a narrower scope of practice; that without pre-requisite experimentation and accountability in guideline implementation there is no sound evidence that hypothesis based on interpretation of evidence with necessarily result in the best and most practice treatment recommendations; that there is a local culture in evidence interpretation that gives rise to (and is presented as) a presumption of unquestionable, accepted dogma; that the treatment recommendation devised by one group (expert or not) based on an interpretation of evidence (a consensus) may not be the only, best, safest or most easily translated into action at user level, recommendation available; that the elevation of treatment recommendations and guidelines (based on restrictive and purely theoretical consensus) to the status of “scientific law” is not scientific; that the methodologies of evidence review that relegates the field of BLS resuscitation practice to being largely based on “poor or very week evidence” is a flawed and inappropriate methodology for this field of science; that despite a claim of strong scientific rigour, resuscitation recommendations are also governed by the same political factors that have corrupted public understanding, acceptance and revelation of truth as every other area of science and this has led to some treatment recommendations that have become canon and are unable to be changed in the face of evidence or simple ambiguity or lack of utility.
If it were possible to remove the other, (non-patient outcome focused) factors from resuscitation guidelines and treatment recommendations, what indeed would the landscape look like? The conclusion raised in this paper is both straightforward and challenging i.e. If long-standing ambiguities are able to still be readily identified in continuing and newly implemented regimes, then the system governing and maintaining these regimes is significantly flawed and misguided. These anomalies are easily identified by anyone who makes more than a cursory review of treatment recommendations and guidelines and serve only to undermine both the methodology used and the factual and established framework.
At the BLS level there are several factors borne out from experience and the evidence:
- The chances of long term survival are maximised in the first 6 minutes of an arrest and this is the pre-ambulance and pre-ACLS period i.e. BLS
- The current simplistic and “universal” protocol is not pragmatically biased to the most common arrest aetiology i.e. Adult SCA. The focus on a young, healthy patient in an arrest caused by hypoxia as the typical occurrence is misguided and not supported by evidence. It is also most likely resulting in decreased survival rates in Adult SCA.
- The multiple steps of the current DRSABCD protocol (designed to cover all scenarios rather than the most common experience) are not retained and able to be accurately and sequentially applied consistently by BLS users in an emergency situation.
- The hierarchical position of defibrillation in the DRSABCD protocol is not reflective of best-practice.
- The notion that BLS users lack the mental capacity and aptitude to manage change and attempt anything outside a short-list determined without evidence must be rejected.
- Many recommendations and erroneous notions have ceased to be debated regardless of their scientific or practical merit. They continue to be regurgitated in successive treatment recommendations and guidelines as unequivocal facts but are never validated.
- Without end-user involvement and testing of recommendations (prior to being “set into law”); treatment recommendations cannot assume the gravity they expect.
- Sciencism can be just as destructive to outcomes as the inadequate methodologies that led to the vacillating recommendations of the past and it can never trump logic or utility.
- The inherent limitations of survival relating to resuscitation practice are not resolved by just doing traditional interventions “better” but by rethinking and challenging the existing dogma and validating the logic on which they are based and results they achieve in actual practice.
The methodology used to develop local guidelines is founded on the notion that all Australian guidelines are “agreed to” by all stakeholders and therefore represent accepted “best practice” is fundamentally flawed and disingenuous. The only decision makers for the determination of content and structure of local guidelines sit at the top of a bureaucratic pyramid. As guidelines are viewed as “edicts from on high” there is little resistance at lower levels and any contrary view or call for change, has no power to affect change against an “expert hierarchy” and is actively dismissed and resisted.
Sciencism and a lack of true utility have been the result of this system as seen by these examples in this paper, however this is not exhaustive. It can be seen that the value of current treatment recommendations and guidelines cannot be accepted on face value alone as although resulting from a formal consensus process, this does not guarantee utility nor that they are any more than opinions based on poor science and entrenched sciencism. Re-enforcing established simplistic (and stylised) treatment recommendations and guidelines, in the absence of evidence of utility cannot realise the quality of outcomes that are possible. The 2017 ILCOR Summary Statement identifies a plethora of fundamental knowledge gaps in CPR practice (summarised down to no less than 18 in the ILCOR document); knowledge gaps that undermine any attempt to formulate credible recommendations, that can be so commonly followed without question.
References
ILCOR Knowledge Gaps and Clinical Research Priorities for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, Circulation 2018
Australian Resuscitation Council Guideline 6 – Compressions, Evidence Worksheet
Australian Resuscitation Council Guideline 6 – Compressions
Australian Resuscitation Council Guideline 9.2.9 – First aid Management of a Diabetic Emergency
2017 International Consensus on Cardiopulmonary Resuscitation and emergency Cardiovascular Care Science with Treatment Recommendations Summary, 2017 ERC and AHA
Minimally Interrupted Cardiac resuscitation by Emergency Medical Services for Out-of-Hospital Cardiac Arrest Bentley J. Bobrow, MD Lani L. Clark, BS Gordon A. Ewy, MD Vatsal Chikani, MPH Arthur B. Sanders, MD Robert A. Berg, MD Peter B. Richman, MD Karl B. Kern, MD, JAMA, March 12, 2008—Vol 299, No. 10
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665060/

Those who follow the Australian Resuscitation Advisory Network, will know that the Australian Resuscitation Council (despite claiming to be a legitimate and professional organisation) has used its influence and all means (fair and foul) to close down any decent or debate on resuscitation in Australia; that does not agree with their opinion and regardless of the evidence. ARAN is not alone and many small organisations involved in some amazing initiatives to improve survival rates in OHCA have suffered from the subversive and destructive influence of the ARC in its quest to retain power and "authority" over thought, discussion, debate and practice in Australia ahead of saving lives.
Ironically this years "Spark of Life" conference has the theme "Resuscitation - it's about time" as ARAN has been advocating for change to the 30 year-old paradigm for several years. There is no doubt that this conference will focus on doing the same thing, but better, rather than anything that challenges the parochial dogma (canon law of resuscitation) in Australia. ARAN has played the game with the ARC (and the other events it has control over), by submitting abstracts for inclusion. Not surprisingly every abstract ever submitted by ARAN has been rejected quickly and most likely without any assessment using the process described in the abstract conditions. To test the political influence in these decisions over the scientific, these have been both controversial subjects that challenge the status quo and purely scientific reports.
Science without challenges and debate is not science. It is rhetoric!
Ironically this years "Spark of Life" conference has the theme "Resuscitation - it's about time" as ARAN has been advocating for change to the 30 year-old paradigm for several years. There is no doubt that this conference will focus on doing the same thing, but better, rather than anything that challenges the parochial dogma (canon law of resuscitation) in Australia. ARAN has played the game with the ARC (and the other events it has control over), by submitting abstracts for inclusion. Not surprisingly every abstract ever submitted by ARAN has been rejected quickly and most likely without any assessment using the process described in the abstract conditions. To test the political influence in these decisions over the scientific, these have been both controversial subjects that challenge the status quo and purely scientific reports.
Science without challenges and debate is not science. It is rhetoric!
A TALE OF TWO TODDLERS
How the absence of post guideline implementation surveillance can lead to adverse outcomes.
A new paper by ARAN highlighting how poor processes and weak science can contribute to premature and preventable deaths. The paper uses two examples of toddlers in Australia who died from airway obstructions, despite application (by training rescuers) of the current ANZCOR guidelines..to no affect. These examples raise serious questions as to the science and accountability of "guidelines" and the dangers of not having a critical review process when measures fail. While medical devices need to have Post Market Surveillance (PMS) systems in place to appropriately identify adverse events, there is no such requirement for ANZCOR guidelines, despite being used by the Industrial Skills Council, across the community to dictate first aid measures in Australia.
How the absence of post guideline implementation surveillance can lead to adverse outcomes.
A new paper by ARAN highlighting how poor processes and weak science can contribute to premature and preventable deaths. The paper uses two examples of toddlers in Australia who died from airway obstructions, despite application (by training rescuers) of the current ANZCOR guidelines..to no affect. These examples raise serious questions as to the science and accountability of "guidelines" and the dangers of not having a critical review process when measures fail. While medical devices need to have Post Market Surveillance (PMS) systems in place to appropriately identify adverse events, there is no such requirement for ANZCOR guidelines, despite being used by the Industrial Skills Council, across the community to dictate first aid measures in Australia.
| a_tale_of_two_toddlers.pdf |
Bystander-initiated conventional vs compression-only cardiopulmonary resuscitation and outcomes after out-of-hospital cardiac arrest due to drowning
Tatsuma Fukuda, Naoko Ohashi-Fukuda, Kei Hayashida, Yutaka Kondo, Ichiro Kukita Resuscitation 2019 August 22
BACKGROUND: Great emphasis has been placed on rescue breathing in out-of-hospital cardiac arrest (OHCA) due to drowning. However, there is no evidence about the effect of rescue breathing on neurologically favorable survival after OHCA due to drowning. The aim of this study is to examine the effect of bystander-initiated conventional (with rescue breathing) versus compression-only (without rescue breathing) cardiopulmonary resuscitation (CPR) in OHCA due to drowning. METHODS: This nationwide population-based observational study using prospectively collected government-led registry data included patients with OHCA due to drowning who were transported to an emergency hospital in Japan between 2013 and 2016. The primary outcome was one-month neurologically favorable survival. RESULTS: The full cohort (n = 5,121) comprised 2,486 (48.5%) male patients, and the mean age was 72.4 years (standard deviation, 21.6). Of these, 968 (18.9%) received conventional CPR, and 4,153 (81.1%) received compression-only CPR. 928 patients receiving conventional CPR were propensity-matched with 928 patients receiving compression-only CPR. In the propensity score-matched cohort, one-month neurologically favorable survival was not significantly different between the two groups (7.5% in the conventional CPR group vs. 6.6% in the compression-only CPR group; risk ratio, 1.15; 95% confidence interval, 0.82-1.60; P = 0.4147). This association was consistent across a variety of subgroup analyses. CONCLUSIONS: Among patients with OHCA due to drowning, there were no differences in one-month neurologically favorable survival between bystander-initiated conventional and compression-only CPR groups, although several important data (e.g., water temperature, submersion duration, or body of water) could not be addressed. Further study is warranted to confirm our findings. to edit.
Head-Up CPR May Improve Neurologically Intact Survival Rates By Johanna Moore, MD, MS | 2.14.19
Head-up CPR is a novel concept in resuscitation that has the potential to improve neurologically intact survival after cardiac arrest.Inspired by the clinical question of whether patients in cardiac arrest should be transported either head-up or feet-up in a small elevator, an initial animal study was performed in 2014. In this swine model of cardiac arrest, pigs underwent five-minute periods of automated CPR with an impedance threshold device (ITD-16) in the traditional supine position, then with a 30-degree whole-body head-up tilt, and then a 30-degree whole-body head-down tilt.
The cerebral blood flow and cerebral perfusion pressures (CerPP) were higher in the whole-body tilt-up group vs. the flat group. Intracranial pressure (ICP) was also lower in the whole-body head-up tilt group. Notably, CerPP and ICP were lower and higher, respectively, in the whole-body head-down tilt.1
Subsequent studies refined the body position over a longer period of CPR, where the head and thorax of the pig was elevated during 22 minutes of active compression-decompression (ACD) CPR plus use of an ITD-16 (ACD+ITD) to reduce venous pooling in the lower extremities during resuscitation. CerPP was higher and sustained over this entire period of time in the ACD+ITD head-up group vs. the flat group.2 (See Figure 1.)
Further studies using a similar protocol for a prolonged period of head-up ACD+ITD CPR showed a doubling of cerebral blood after 15 minutes of CPR and also replicated the finding of higher CerPP pressures seen in previous studies.3
The primary mechanism of benefit behind head-up CPR is the use of gravity to enhance venous drainage not only from the brain and cerebral venous sinuses, but also the paravertebral venous plexus, thereby decreasing ICP and creating potential for the forward flow of blood.1,3,4
A secondary mechanism of benefit is thought to be the concept of decreasing the pressure transmitted to the brain via both the venous and arterial vasculature during CPR, effectively reducing a concussive injury with compression.
A third mechanism involves redistributing blood flow through the lungs in a manner similar to what occurs when patients with heart failure sit upright.
Animal studies show head-up CPR is dependent on circulatory adjuncts during CPR, such as the ITD-16 to drive blood “uphill” to maintain an adequate mean arterial blood pressure during resuscitation. When head-up standard CPR is performed, CerPP during resuscitation has been reported in the range of 7–10% of baseline CerPP values.2,5 This is compared to 50–60% of baseline CerPP values when head-up CPR is performed with circulatory adjuncts, such as ACD+ITD CPR or CPR performed with both the LUCAS mechanical chest compression device combined with use of the ITD-16.1–3
Other important considerations when performing head-up CPR includes: performing CPR flat before elevation, which primes the cardio-cerebral circuit; and to use caution when elevating the entire body over a long CPR effort, as blood likely pools in the lower extremities over time.6,7
The finding of lowered ICP and higher CerPP with head-up CPR has subsequently been replicated in a human cadaver model, the strongest translational evidence to date that head-up CPR is ready to move forward into humans in active cardiac arrest.8
More recent animal studies have focused on the optimal head-up CPR height and timing of head and thorax elevation. To date, no optimal angle has been determined,however a sequence effect has emerged, where animals treated with a controlled progressive elevation after two minutes of “priming”—to a final head height of 22 cm and a heart height of 9 cm—had sustained CerPPs and also higher coronary perfusion pressures > 70% of baseline values after > 15 minutes of ACD+ITD CPR.9,10
Most recently, head-up CPR has been incorporated into bundles of care in Palm Beach County, Fla., and Rialto, Calif.
As part of these bundles, survival rates in these two EMS systems have essentially doubled. Head-up CPR, when applied correctly and as part of a bundle of care, has the potential to improve neurologically intact survival rates after cardiac arrest.
References1. Debaty G, Shin SD, Metzger A, et al. Tilting for perfusion: Head-up position during cardiopulmonary resuscitation improves brain flow in a porcine model of cardiac arrest. Resuscitation. 2015;87:38–43.
2. Ryu HH, Moore JC, Yannopoulos D, et al. The effect of head up cardiopulmonary resuscitation on cerebral and systemic hemodynamics. Resuscitation. 2016;102:29–34.
3. Moore JC, Segal N, Lick MC, et al. Head and thorax elevation during active compression decompression cardiopulmonary resuscitation with an impedance threshold device improves cerebral perfusion in a swine model of prolonged cardiac arrest. Resuscitation. 2017;121:195–200.
4. Guerci AD, Shi AY, Levin H, et al. Transmission of intrathoracic pressure to the intracranial space during cardiopulmonary resuscitation in dogs. Circ Res. 1985;56(1):20–30.
5. Putzer G, Braun P, Martini J, et al. Effects of head-up vs. supine CPR on cerebral oxygenation and cerebral metabolism—A prospective, randomized porcine study. Resuscitation. 2018;128:51–55.
6. Park YJ, Shin SD, Song KJ, et al. Abstract 18341: Worsened survival with head-up positional cardiopulmonary resuscitation in a porcine cardiac arrest model. Circulation. 2016;134(Suppl 1):A18341.
7. Moore JC, Segal N, Debaty G, et al. The “do’s and don’ts” of head up CPR: Lessons learned from the animal laboratory. Resuscitation. 2018;129:e6–e7.
8. Moore JC, Holley J, Segal N, et al. Consistent head up cardiopulmonary resuscitation haemodynamics are observed across porcine and human cadaver translational models. Resuscitation. 2018;132:133–139.
9. Moore JC, Salverda B, Lick M, et al. Abstract 17: Controlled progressive elevation maximizes cerebral perfusion pressure during head up CPR in a swine model of cardiac arrest. Circulation. 2018;138(Suppl 2):A17.
10. Rojas-Salvador C, Moore J, Salverda B, et al. Controlled fast head and thorax elevation improves cerebral perfusion pressure during active compression and decompression CPR with an impedance threshold device in a porcine model of cardiac arrest. [Abstract #35.] in Berry C, Kupas D, Olaf M, et al. Abstracts for the 2019 NAEMSP Scientific Assembly. Prehosp Emerg Care. 2018:1-251.
it.
Head-up CPR is a novel concept in resuscitation that has the potential to improve neurologically intact survival after cardiac arrest.Inspired by the clinical question of whether patients in cardiac arrest should be transported either head-up or feet-up in a small elevator, an initial animal study was performed in 2014. In this swine model of cardiac arrest, pigs underwent five-minute periods of automated CPR with an impedance threshold device (ITD-16) in the traditional supine position, then with a 30-degree whole-body head-up tilt, and then a 30-degree whole-body head-down tilt.
The cerebral blood flow and cerebral perfusion pressures (CerPP) were higher in the whole-body tilt-up group vs. the flat group. Intracranial pressure (ICP) was also lower in the whole-body head-up tilt group. Notably, CerPP and ICP were lower and higher, respectively, in the whole-body head-down tilt.1
Subsequent studies refined the body position over a longer period of CPR, where the head and thorax of the pig was elevated during 22 minutes of active compression-decompression (ACD) CPR plus use of an ITD-16 (ACD+ITD) to reduce venous pooling in the lower extremities during resuscitation. CerPP was higher and sustained over this entire period of time in the ACD+ITD head-up group vs. the flat group.2 (See Figure 1.)
Further studies using a similar protocol for a prolonged period of head-up ACD+ITD CPR showed a doubling of cerebral blood after 15 minutes of CPR and also replicated the finding of higher CerPP pressures seen in previous studies.3
The primary mechanism of benefit behind head-up CPR is the use of gravity to enhance venous drainage not only from the brain and cerebral venous sinuses, but also the paravertebral venous plexus, thereby decreasing ICP and creating potential for the forward flow of blood.1,3,4
A secondary mechanism of benefit is thought to be the concept of decreasing the pressure transmitted to the brain via both the venous and arterial vasculature during CPR, effectively reducing a concussive injury with compression.
A third mechanism involves redistributing blood flow through the lungs in a manner similar to what occurs when patients with heart failure sit upright.
Animal studies show head-up CPR is dependent on circulatory adjuncts during CPR, such as the ITD-16 to drive blood “uphill” to maintain an adequate mean arterial blood pressure during resuscitation. When head-up standard CPR is performed, CerPP during resuscitation has been reported in the range of 7–10% of baseline CerPP values.2,5 This is compared to 50–60% of baseline CerPP values when head-up CPR is performed with circulatory adjuncts, such as ACD+ITD CPR or CPR performed with both the LUCAS mechanical chest compression device combined with use of the ITD-16.1–3
Other important considerations when performing head-up CPR includes: performing CPR flat before elevation, which primes the cardio-cerebral circuit; and to use caution when elevating the entire body over a long CPR effort, as blood likely pools in the lower extremities over time.6,7
The finding of lowered ICP and higher CerPP with head-up CPR has subsequently been replicated in a human cadaver model, the strongest translational evidence to date that head-up CPR is ready to move forward into humans in active cardiac arrest.8
More recent animal studies have focused on the optimal head-up CPR height and timing of head and thorax elevation. To date, no optimal angle has been determined,however a sequence effect has emerged, where animals treated with a controlled progressive elevation after two minutes of “priming”—to a final head height of 22 cm and a heart height of 9 cm—had sustained CerPPs and also higher coronary perfusion pressures > 70% of baseline values after > 15 minutes of ACD+ITD CPR.9,10
Most recently, head-up CPR has been incorporated into bundles of care in Palm Beach County, Fla., and Rialto, Calif.
As part of these bundles, survival rates in these two EMS systems have essentially doubled. Head-up CPR, when applied correctly and as part of a bundle of care, has the potential to improve neurologically intact survival rates after cardiac arrest.
References1. Debaty G, Shin SD, Metzger A, et al. Tilting for perfusion: Head-up position during cardiopulmonary resuscitation improves brain flow in a porcine model of cardiac arrest. Resuscitation. 2015;87:38–43.
2. Ryu HH, Moore JC, Yannopoulos D, et al. The effect of head up cardiopulmonary resuscitation on cerebral and systemic hemodynamics. Resuscitation. 2016;102:29–34.
3. Moore JC, Segal N, Lick MC, et al. Head and thorax elevation during active compression decompression cardiopulmonary resuscitation with an impedance threshold device improves cerebral perfusion in a swine model of prolonged cardiac arrest. Resuscitation. 2017;121:195–200.
4. Guerci AD, Shi AY, Levin H, et al. Transmission of intrathoracic pressure to the intracranial space during cardiopulmonary resuscitation in dogs. Circ Res. 1985;56(1):20–30.
5. Putzer G, Braun P, Martini J, et al. Effects of head-up vs. supine CPR on cerebral oxygenation and cerebral metabolism—A prospective, randomized porcine study. Resuscitation. 2018;128:51–55.
6. Park YJ, Shin SD, Song KJ, et al. Abstract 18341: Worsened survival with head-up positional cardiopulmonary resuscitation in a porcine cardiac arrest model. Circulation. 2016;134(Suppl 1):A18341.
7. Moore JC, Segal N, Debaty G, et al. The “do’s and don’ts” of head up CPR: Lessons learned from the animal laboratory. Resuscitation. 2018;129:e6–e7.
8. Moore JC, Holley J, Segal N, et al. Consistent head up cardiopulmonary resuscitation haemodynamics are observed across porcine and human cadaver translational models. Resuscitation. 2018;132:133–139.
9. Moore JC, Salverda B, Lick M, et al. Abstract 17: Controlled progressive elevation maximizes cerebral perfusion pressure during head up CPR in a swine model of cardiac arrest. Circulation. 2018;138(Suppl 2):A17.
10. Rojas-Salvador C, Moore J, Salverda B, et al. Controlled fast head and thorax elevation improves cerebral perfusion pressure during active compression and decompression CPR with an impedance threshold device in a porcine model of cardiac arrest. [Abstract #35.] in Berry C, Kupas D, Olaf M, et al. Abstracts for the 2019 NAEMSP Scientific Assembly. Prehosp Emerg Care. 2018:1-251.
it.
Strategies to improve survival outcomes of out-of-hospital cardiac arrest (OHCA) given a fixed budget: A simulation study.
lY.WeiaP.P.PekbcB.DoblecE.A.FinkelsteincW.WahdY.Y.NgefS.O.CheahgM.Y.C.ChiafB.S.H.LeonghH.N.GaniD.R.H.MaojL.P.ThamkS.Fook-ChonglM.E.H.Ongbc
Background Our study aimed to identify a strategy that maximizes survival upon hospital discharge or 30-days post out-of-hospital cardiac arrest (OHCA) in Singapore for fixed investments of S$1, S$5, or S$10 million. Four strategies were compared: (1) no additional investment; (2) reducing response time via leasing of more ambulances; (3) increasing number of people trained in cardiopulmonary resuscitation (CPR); and (4) automated external defibrillators (AED).
Methods We estimated the effect of ambulance response time, bystander CPR and AED on survival based on Singapore’s 2010-2015 OHCA registry data. We simulated the changes in ambulance response times and likelihood of 1) CPR and 2) AED usage as a function of their increased availability, which was then combined with the effect of each factor to determine the increase in survival for each strategy.
Results Survival given no additional investment was 4.03% (95% CI: 3.96%, 4.10%). The investments in ambulances, CPR training and AEDs for a given budget of S$1 M changed survival to 4.03% (95% CI: 3.96%, 4.10%), 4.04% (95% CI: 3.98%, 4.11%), and 4.44% (95% CI: 4.35%, 4.54%), respectively. This generated 0, 2 and 102 additional life years saved respectively. Given a budget of S$5 M or S$10 M, 509 or 886 additional life years could be saved, by investing in an additional 10,000 or 20,000 AEDs respectively. The strategies reached a saturation effect whereby improvement in survival was marginal when the budget was increased to ≥ S$5 M for investment in ambulances and CPR training.
Conclusions Investing in AEDs had the most gain in survival.
lY.WeiaP.P.PekbcB.DoblecE.A.FinkelsteincW.WahdY.Y.NgefS.O.CheahgM.Y.C.ChiafB.S.H.LeonghH.N.GaniD.R.H.MaojL.P.ThamkS.Fook-ChonglM.E.H.Ongbc
Background Our study aimed to identify a strategy that maximizes survival upon hospital discharge or 30-days post out-of-hospital cardiac arrest (OHCA) in Singapore for fixed investments of S$1, S$5, or S$10 million. Four strategies were compared: (1) no additional investment; (2) reducing response time via leasing of more ambulances; (3) increasing number of people trained in cardiopulmonary resuscitation (CPR); and (4) automated external defibrillators (AED).
Methods We estimated the effect of ambulance response time, bystander CPR and AED on survival based on Singapore’s 2010-2015 OHCA registry data. We simulated the changes in ambulance response times and likelihood of 1) CPR and 2) AED usage as a function of their increased availability, which was then combined with the effect of each factor to determine the increase in survival for each strategy.
Results Survival given no additional investment was 4.03% (95% CI: 3.96%, 4.10%). The investments in ambulances, CPR training and AEDs for a given budget of S$1 M changed survival to 4.03% (95% CI: 3.96%, 4.10%), 4.04% (95% CI: 3.98%, 4.11%), and 4.44% (95% CI: 4.35%, 4.54%), respectively. This generated 0, 2 and 102 additional life years saved respectively. Given a budget of S$5 M or S$10 M, 509 or 886 additional life years could be saved, by investing in an additional 10,000 or 20,000 AEDs respectively. The strategies reached a saturation effect whereby improvement in survival was marginal when the budget was increased to ≥ S$5 M for investment in ambulances and CPR training.
Conclusions Investing in AEDs had the most gain in survival.
Providing the best chest compression quality: Standard CPR versus chest compressions only in a bystander resuscitation model
Bernhard Rössler, Julius Goschin, Mathias Maleczek, Felix Piringer, Rainer Thell, Martina Mittlböck, Karl Schebesta
PloS One 2020, 15 (2): e0228702
AIM OF THE STUDY: Bystander-initiated basic life support (BLS) for the treatment of prehospital cardiac arrest increases survival but is frequently not performed due to fear and a lack of knowledge. A simple flowchart can improve motivation and the quality of performance. Furthermore, guidelines do recommend a chest compression (CC)-only algorithm for dispatcher-assisted bystander resuscitation, which may lead to increased fatigue and a loss of compression depth. Consequently, we wanted to test the hypothesis that CCs are more correctly delivered in a flowchart-assisted standard resuscitation algorithm than in a CC-only algorithm.
METHODS: With the use of a manikin model, 84 laypersons were randomized to perform either flowchart-assisted standard resuscitation or CC-only resuscitation for 5min. The primary outcome was the total number of CCs.
RESULTS: The total number of correct CCs did not significantly differ between the CC-only group and the standard group (63 [±81] vs. 79 [±86]; p = 0.394; 95% CI of difference: 21-53). The total hand-off time was significantly lower in the CC-only group than in the standard BLS group. The relative number of correct CCs (the fraction of the total number of CCs achieving 5-6cm) and the level of exhaustion after BLS did not significantly differ between the groups.
CONCLUSION: Standard BLS did not lead to an increase in correctly delivered CCs compared to CC-only resuscitation and exhibited significantly more hand-off time. The low rate of CCs in both groups indicates the need for an increased focus on performance during BLS training.
i
Bernhard Rössler, Julius Goschin, Mathias Maleczek, Felix Piringer, Rainer Thell, Martina Mittlböck, Karl Schebesta
PloS One 2020, 15 (2): e0228702
AIM OF THE STUDY: Bystander-initiated basic life support (BLS) for the treatment of prehospital cardiac arrest increases survival but is frequently not performed due to fear and a lack of knowledge. A simple flowchart can improve motivation and the quality of performance. Furthermore, guidelines do recommend a chest compression (CC)-only algorithm for dispatcher-assisted bystander resuscitation, which may lead to increased fatigue and a loss of compression depth. Consequently, we wanted to test the hypothesis that CCs are more correctly delivered in a flowchart-assisted standard resuscitation algorithm than in a CC-only algorithm.
METHODS: With the use of a manikin model, 84 laypersons were randomized to perform either flowchart-assisted standard resuscitation or CC-only resuscitation for 5min. The primary outcome was the total number of CCs.
RESULTS: The total number of correct CCs did not significantly differ between the CC-only group and the standard group (63 [±81] vs. 79 [±86]; p = 0.394; 95% CI of difference: 21-53). The total hand-off time was significantly lower in the CC-only group than in the standard BLS group. The relative number of correct CCs (the fraction of the total number of CCs achieving 5-6cm) and the level of exhaustion after BLS did not significantly differ between the groups.
CONCLUSION: Standard BLS did not lead to an increase in correctly delivered CCs compared to CC-only resuscitation and exhibited significantly more hand-off time. The low rate of CCs in both groups indicates the need for an increased focus on performance during BLS training.
i
Comparing the two-finger versus two-thumb technique for single person infant CPR: A systematic review and meta-analysis
Michael G. Millina,,Correspondence information about the author Michael G. MillinEmail the author Michael G. Millin
, David Bogumilb , Jennifer N. Fishec Rita V. Burked
Introduction
Current guidelines recommend that single person cardiopulmonary resuscitation (CPR) on an infant should be performed with two-fingers just below the inter-mammillary line with the hand clenched, while two-person CPR should be performed with two-thumbs with the hands encircling the chest. Those recommendations are based on literature that demonstrates higher quality chest compressions with the two-thumb technique, with concerns that this technique may compromise ventilation parameters when performed by the single rescuer. The purpose of this study is to compare the two compression techniques’ performance during CPR using both compression and ventilation parameters.
Methods
We performed a systematic review and meta-analysis of literature identified through a search of PubMed and One-Search comparing the quality of chest compressions and ventilation parameters between the two-thumb and two-finger techniques (Prospero registration # CRD42018087672).
Results
We identified 20 manuscripts examining single person infant CPR that met study criteria, with 16 that included data suitable for meta-analysis. All of the studies included in the analysis were performed on a standardized manikin. Overall, the two-thumb technique resulted in a mean difference of 5.61 mm greater compression depth compared to the two-finger technique, with 36.91% more compressions of adequate depth per national guidelines. Interestingly, ventilation parameters did not differ between the two techniques.
Conclusion
While recognizing that the results of this review may differ from actual clinical experience due to the lack of fidelity between manikins and actual human infants, this systematic review with meta-analysis demonstrates that when CPR is performed on a simulated infant manikin by a single rescuer, the two-thumb technique with hands encircling the chest improves chest compression quality and does not appear to compromise ventilation.